Orthodontics places very different demands on digital impressions than most other dental disciplines. When we talk about an intraoral scanner for orthodontics, we are not simply replacing alginate with a camera we are replacing a full-arch diagnostic record that guides tooth movement over months or years. Every rotation, torque adjustment, space closure plan, and aligner stage depends on the accuracy of that initial scan. A few hundred microns of deviation across the arch may seem minor, but in orthodontic biomechanics it can translate into poor aligner fit, inaccurate bracket positioning, or extended treatment time.
Over the past decade, intraoral scanning in orthodontics has shifted from being a novelty to becoming a central diagnostic and planning tool. Yet orthodontics adopted digital scanning later than prosthodontics for a reason: full-arch capture, crowded dentition, reflective bracket surfaces, and continuous treatment monitoring create technical challenges that single-crown workflows simply do not face. Understanding how these scanners perform under orthodontic conditions rather than in ideal laboratory settings is what truly determines whether an intraoral scanner in orthodontics becomes a clinical asset or an expensive device that rarely leaves its cart.
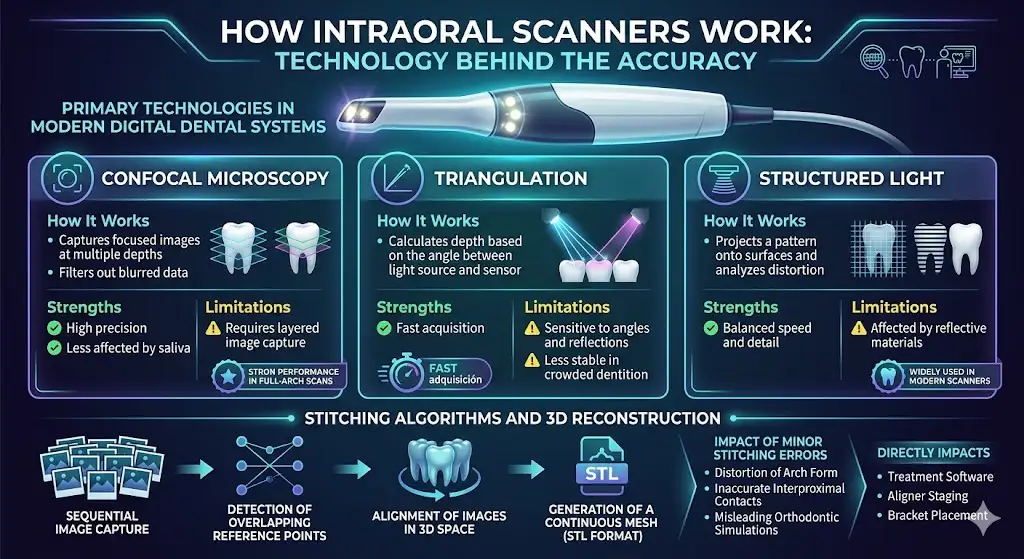
How Intraoral Scanners Work: Technology Behind the Accuracy
Confocal Microscopy vs Triangulation vs Structured Light
At the core of every intraoral scanner for orthodontics is an optical system that captures thousands of images and converts them into a precise 3D model. The final accuracy is not determined by hardware alone it depends on how light interacts with enamel, soft tissue, and reflective surfaces, and how that data is processed.
Three primary technologies are used in modern digital dental impression systems:
| Technology | How It Works | Strengths | Limitations | Relevance in Orthodontics |
| Confocal Microscopy | Captures focused images at multiple depths and filters out blurred data | High precision, less affected by saliva | Requires layered image capture | Strong performance in full-arch scans |
| Triangulation | Calculates depth based on the angle between light source and sensor | Fast acquisition | Sensitive to angles and reflections | Less stable in crowded dentition |
| Structured Light | Projects a pattern onto surfaces and analyzes distortion | Balanced speed and detail | Affected by reflective materials | Widely used in modern scanners |
From a clinical standpoint, the key factor is not just resolution, but scan accuracy at the micron level across a full arch.
Stitching Algorithms and 3D Reconstruction
Raw image capture is only the first step. Every intraoral scanning orthodontics system relies on stitching algorithms to merge hundreds or thousands of frames into a single continuous 3D model.
The workflow typically follows:
- Sequential image capture
- Detection of overlapping reference points
- Alignment of images in 3D space
- Generation of a continuous mesh (usually STL format)
Even minor stitching errors can result in:
- Distortion of arch form
- Inaccurate interproximal contacts
- Misleading orthodontic simulations
“Errors in image stitching can accumulate over long-span scans, particularly in full-arch acquisitions.”
https://www.mdpi.com/1660-4601/19/3/1407
In orthodontics, this directly impacts:
- orthodontic treatment planning software
- aligner staging accuracy
- bracket positioning precision
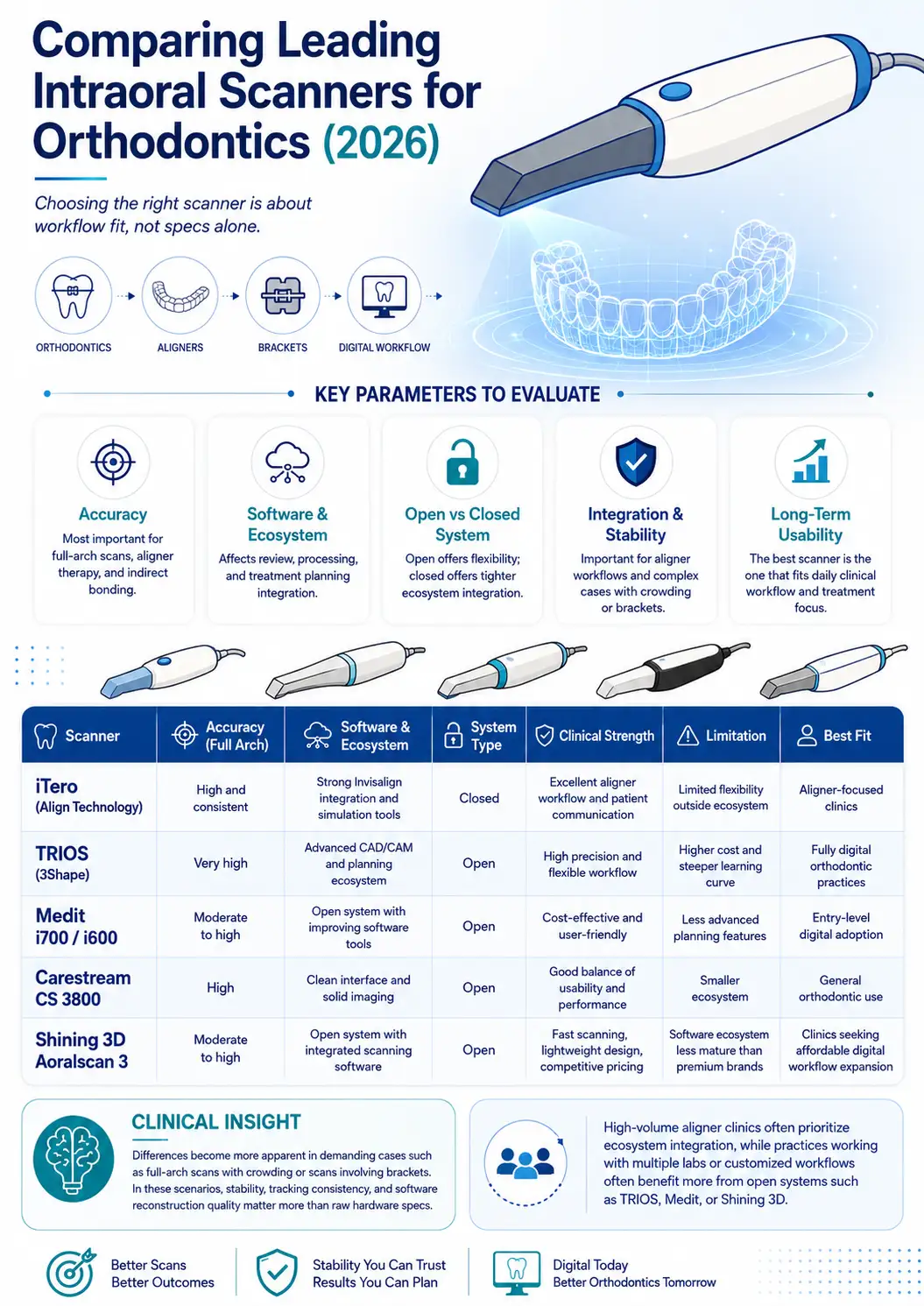
Comparing Leading Intraoral Scanners for Orthodontics (2026)
Key Parameters to Evaluate
Selecting the best intraoral scanner for orthodontists requires a broader perspective than simply comparing specifications. The decision should be based on how well the scanner integrates into the clinical and business workflow of the practice.
Accuracy remains the most important factor, particularly for full-arch scans used in aligner therapy and indirect bonding. However, software capabilities are equally influential, as they determine how easily scans can be processed, reviewed, and transferred into treatment planning systems. Another key consideration is whether the system is open or closed. Open systems allow greater flexibility in choosing laboratories and software, while closed systems may offer tighter integration with specific treatment ecosystems.
Integration with aligner providers, scanning stability in complex cases, and long-term usability should also be considered. In many cases, the “best” scanner is not the one with the highest technical specifications, but the one that fits seamlessly into the clinic’s daily workflow and treatment focus.
Brand-Level Overview and Comparison Table
A practical comparison of widely used systems in intraoral scanner orthodontics highlights how different devices serve different clinical priorities rather than competing on a single performance metric.
| Scanner | Accuracy (Full Arch) | Software & Ecosystem | System Type | Clinical Strength | Limitation | Best Fit |
| iTero (Align Technology) | High and consistent | Strong Invisalign integration and simulation tools | Closed | Excellent aligner workflow and patient communication | Limited flexibility outside ecosystem | Aligner-focused clinics |
| TRIOS (3Shape) | Very high | Advanced CAD/CAM and planning ecosystem | Open | High precision and flexible workflow | Higher cost and steeper learning curve | Fully digital orthodontic practices |
| Medit i700 / i600 | Moderate to high | Open system with improving software tools | Open | Cost-effective and user-friendly | Less advanced planning features | Entry-level digital adoption |
| Carestream CS 3800 | High | Clean interface and solid imaging | Open | Good balance of usability and performance | Smaller ecosystem | General orthodontic use |
| Shining 3D Aoralscan 3 | Moderate to high | Open system with integrated scanning software | Open | Fast scanning, lightweight design, competitive pricing | Software ecosystem less mature than premium brands | Clinics seeking affordable digital workflow expansion |
From a clinical standpoint, differences between scanners become more apparent in demanding scenarios such as full-arch scans with crowding or cases involving brackets. In these situations, stability, tracking consistency, and software reconstruction quality have a greater impact than raw hardware specifications.
Clinical insight:
Clinics focused on high-volume aligner cases often prioritize ecosystem integration, while practices working with multiple labs or customized workflows tend to benefit more from open systems like TRIOS, Medit, or Shining 3D.
Clinical Accuracy of Intraoral Scanners in Orthodontics
In Vivo vs In Vitro Accuracy Studies
One of the most common misconceptions is relying solely on laboratory data. In reality, in vivo scanning accuracy determines clinical success.
Reported deviations:
| Condition | Average Deviation |
| In vitro (lab conditions) | 20–40 microns |
| In vivo (clinical conditions) | 50–150 microns |
Factors affecting real-world accuracy:
- Saliva and moisture contamination
- Patient movement
- Limited access in posterior regions
- Soft tissue interference
Important note:
Even the most advanced intraoral scanner in orthodontics can produce inconsistent results if the operator lacks experience or follows an inefficient scanning path.
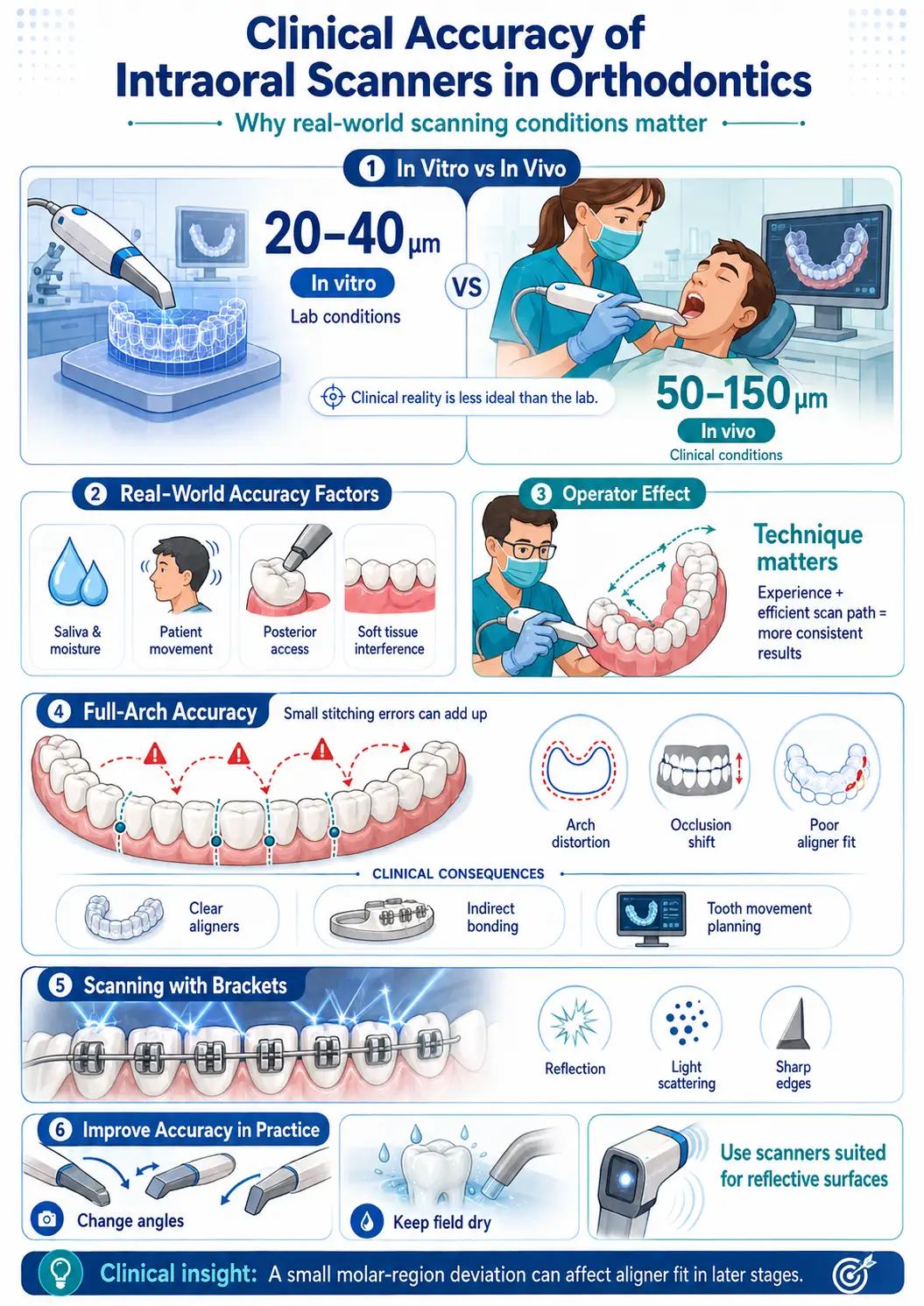
Full-Arch Accuracy: Why It Matters in Orthodontics
Unlike restorative dentistry, orthodontics depends heavily on full-arch scan orthodontics.
The primary issue is cumulative error.
Each stitched frame introduces a small deviation. Across a full arch:
- Errors accumulate progressively
- Arch length can become distorted
- Digital occlusion may shift
This becomes clinically critical in:
- Clear aligner therapy
- Indirect bonding trays
- Long-span tooth movement planning
Clinical insight:
In one aligner case, a minor deviation in the molar region led to poor fit starting at stage 6. The root cause was traced back to the initial scan not the aligner manufacturing.
Scanning with Brackets and Fixed Appliances
Scanning teeth with brackets introduces a different level of complexity.
Key challenges:
- Reflection from metal brackets
- Light scattering
- Difficulty detecting sharp edges
These factors directly affect orthodontic bracket scanning accuracy.
Practical strategies to improve results:
- Adjust scanning angles continuously
- Maintain a dry field
- Use scanners with better performance on reflective surfaces
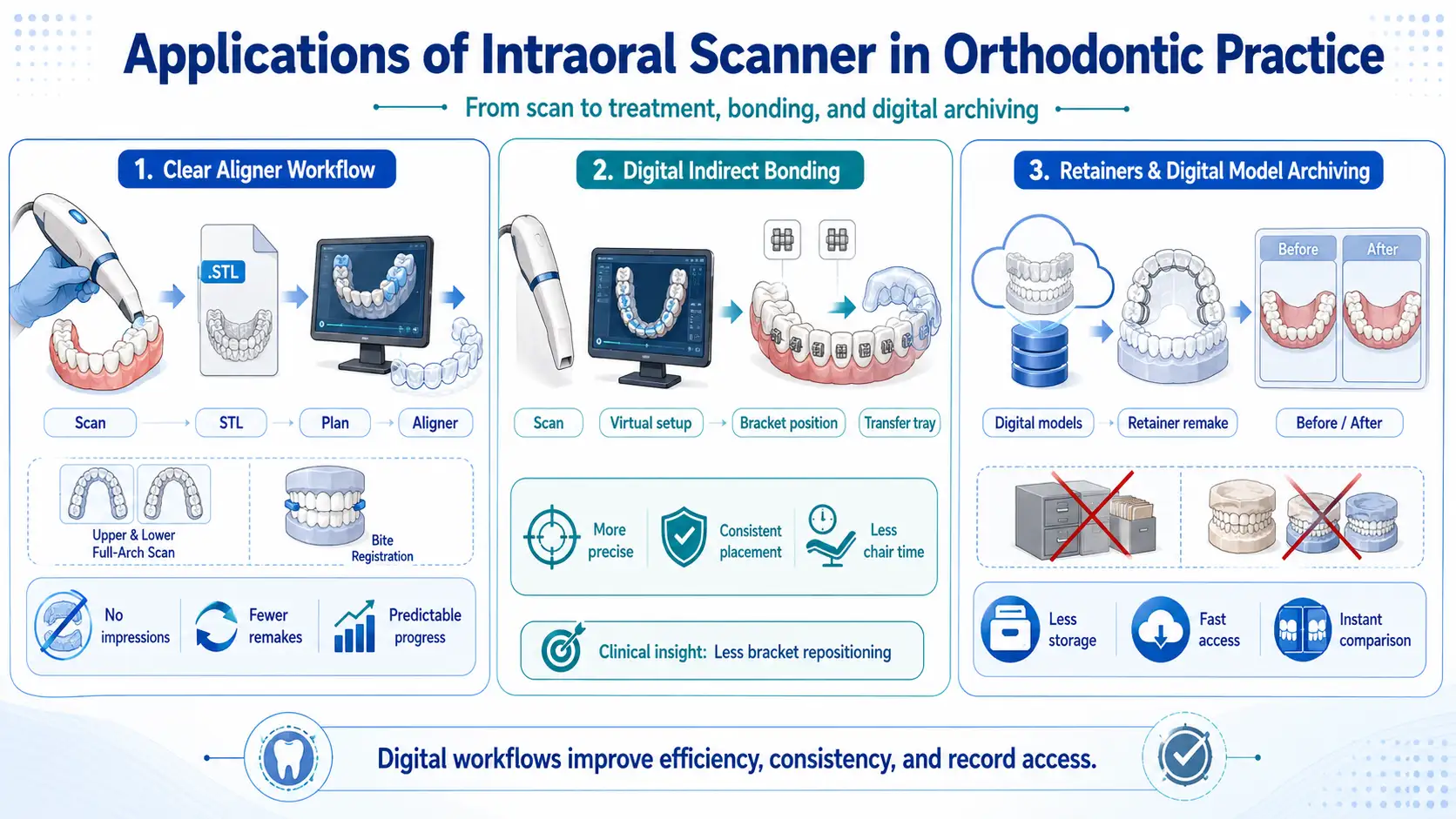
Applications of Intraoral Scanner in Orthodontic Practice
Clear Aligner Workflow
One of the most important applications of intraoral scanning for clear aligners is the fully digital workflow:
Scan → STL → Treatment Planning → Aligner Manufacturing
Typical clinical steps:
- Full-arch scan (upper and lower)
- Bite registration
- STL file generation
- Transfer to planning software or lab
- Staging design
- Aligner production
Key advantages:
- Elimination of traditional impressions
- Reduced need for remakes
- More predictable treatment progression
Digital Indirect Bonding
In indirect bonding digital technique, scan accuracy directly affects bracket positioning.
Workflow:
Scan → Virtual setup → Bracket positioning → Transfer tray fabrication
Clinical benefits:
- Reduced manual positioning errors
- More consistent bracket placement
- Shorter chairside time
Clinical insight:
In cases where digital indirect bonding is used, the need for bracket repositioning is noticeably reduced compared to conventional methods.
Retainers and Digital Model Archiving
A frequently underestimated application is the use of digital orthodontic models.
With digital scans:
- Physical plaster models are no longer required
- Retainers can be reproduced at any time
- Pre- and post-treatment comparisons are instantly available
For clinics, this means:
- Reduced storage requirements
- Faster access to patient records
Clinical Efficiency: Chairside Time, Patient Comfort, and Learning Curve
Time Comparison vs Conventional Impressions
Clinical efficiency is one of the main drivers behind adopting an intraoral scanner for orthodontics, but the real advantage becomes clear when the entire workflow is evaluated rather than just the scanning step. While the actual scan may only save a few minutes compared to traditional impressions, the elimination of material preparation, disinfection, and physical shipping creates a much shorter and more predictable process overall.
| Workflow Step | Conventional Impression | Intraoral Scanning |
| Preparation | Tray selection, material mixing | Scanner setup |
| Capture Time | 3–6 minutes | 2–5 minutes |
| Retakes | Common (distortion, bubbles) | Instant correction |
| Disinfection & Shipping | Required | Not required |
| Lab Communication | Physical | Instant digital transfer |
| Total Chairside Time | 10–15 minutes | 5–8 minutes |
Over the course of a full clinical day, this difference compounds. Instead of dealing with remakes and delays, the orthodontist works with immediate, usable data. In practice, the biggest gain is not speed, but consistency and reduced interruptions in the workflow.
Clinical insight:
The efficiency improvement becomes most noticeable in high-volume aligner practices, where even small time savings per patient translate into a meaningful increase in daily capacity.
Patient Experience and Acceptance
Patient comfort is often underestimated when evaluating intraoral scanning orthodontics, yet it directly influences treatment acceptance and overall experience. Traditional impressions are frequently associated with discomfort, particularly due to gag reflex and the feeling of material filling the mouth. This is especially problematic in younger patients or those with anxiety.
Digital scanning changes this interaction completely. The process is less invasive, can be paused at any time, and allows patients to remain more relaxed during the appointment. Another important aspect is visualization patients can immediately see a 3D model of their teeth, which helps them better understand their condition and proposed treatment.
“Patients reported significantly higher comfort levels with digital impressions compared to conventional methods.”
https://pmc.ncbi.nlm.nih.gov/articles/PMC8834929/
In many clinics, this shift has a measurable effect on case acceptance, particularly for clear aligner treatments where patients expect a modern, technology-driven experience.
Operator Experience and Training Curve
The effectiveness of an intraoral scanner in orthodontics is closely tied to the operator’s technique. Unlike traditional impressions, which are relatively standardized, scanning requires controlled movement, a consistent path, and an understanding of how the software builds the model in real time.
Most clinicians initially experience issues such as losing tracking during full-arch scans or unintentionally introducing distortions by overscanning certain areas. These challenges are not related to the device itself but to how it is used. With regular use, operators develop a more structured scanning approach, leading to more predictable outcomes.
In practical terms, basic proficiency is typically achieved within the first couple of weeks, while consistent full-arch accuracy may take a month or more. As familiarity increases, scanning becomes faster and more reliable, and the likelihood of needing rescans decreases significantly.
Clinical insight:
Once a standardized scanning protocol is established within a clinic, variability between operators drops noticeably, improving overall data quality.
Integration into Digital Orthodontic Workflow
STL Export and CAD/CAM Compatibility
One of the most practical advantages of intraoral scanning for orthodontics is the ability to generate STL files that can be used across different platforms. This allows orthodontists to move beyond single-vendor workflows and collaborate with various laboratories or software providers.
In daily practice, this flexibility simplifies appliance design and enables more customized treatment approaches. Instead of being restricted to predefined systems, clinicians can adapt their workflow based on the specific needs of each case.
Integration with 3D Printing
The connection between intraoral scanning orthodontics and 3D printing has become a central part of modern orthodontic workflows. Once a scan is captured, it can be directly converted into a printable model, which is then used for fabricating aligners, retainers, or indirect bonding trays.
This reduces turnaround time significantly compared to traditional lab processes. Clinics that incorporate in-house printing gain additional control over production timelines and can respond more quickly to adjustments during treatment.
Cloud-Based Case Monitoring
Cloud-based systems extend the value of digital scans beyond initial capture. They allow orthodontists to store, access, and share patient data from different locations, making collaboration with labs or colleagues more efficient.
Over time, this also creates a structured digital archive of cases, enabling easier comparison between treatment stages. For long-term orthodontic treatments, having immediate access to historical data improves both monitoring and decision-making.
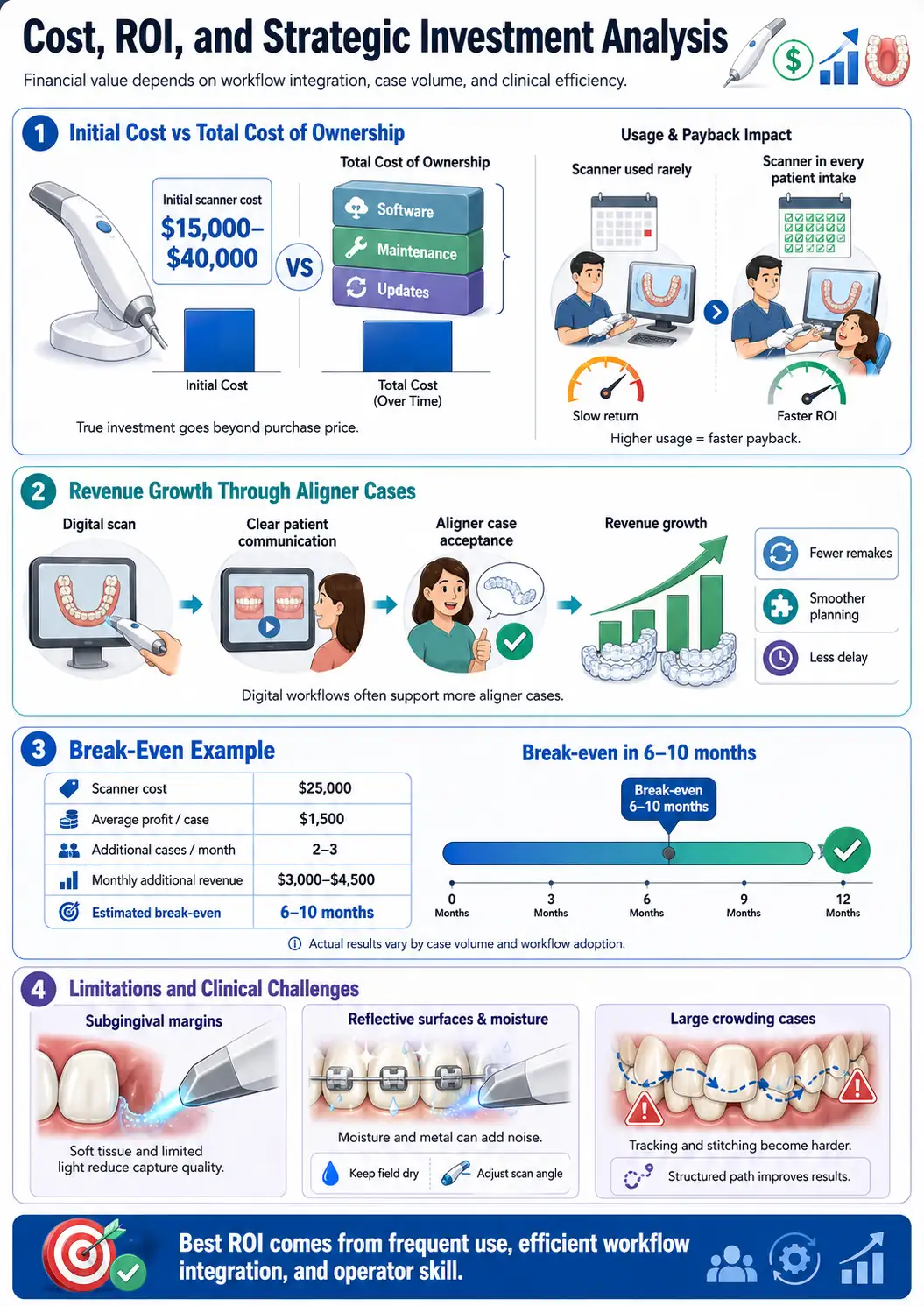
Cost, ROI, and Strategic Investment Analysis
- Initial Cost vs Total Cost of Ownership
Investing in an intraoral scanner for orthodontics involves more than the initial purchase price. While the device itself typically ranges from $15,000 to $40,000, additional factors such as software subscriptions, maintenance, and updates contribute to the total cost over time.
The financial impact depends heavily on how frequently the scanner is used and how well it is integrated into the clinic’s workflow. A scanner that is used only occasionally will have a much longer return period compared to one that becomes part of every patient intake.
- Revenue Increase Through Aligner Cases
Digital workflows are closely tied to the growth of aligner-based treatments. By using intraoral scanning orthodontics, clinicians can simplify the intake process, improve communication with patients, and reduce delays associated with traditional impressions.
This often leads to higher case acceptance, particularly among patients who are already considering aligner therapy. In addition, fewer remakes and more predictable treatment planning contribute to a smoother overall process, which indirectly supports revenue growth.
- Break-Even Analysis for Orthodontic Clinics
A simplified financial model helps illustrate how quickly an intraoral scanner in orthodontics can pay for itself:
| Factor | Example Value |
| Scanner Cost | $25,000 |
| Average Profit per Case | $1,500 |
| Additional Cases per Month | 2–3 |
| Monthly Additional Revenue | $3,000 – $4,500 |
| Estimated Break-Even | 6–10 months |
This model assumes that the scanner contributes to improved efficiency and increased patient acceptance. In reality, the break-even point varies depending on case volume and how effectively the technology is integrated into daily operations.
Limitations and Clinical Challenges
Scanning Subgingival Margins
Although orthodontics does not rely heavily on subgingival detail, there are situations where precise surface capture becomes important, such as attachment design or detailed morphology analysis. In these cases, soft tissue interference and limited light penetration can reduce scan quality, requiring careful technique and sometimes minor adjustments in scanning strategy.
Reflective Surfaces and Moisture
Moisture control remains a consistent challenge in intraoral scanner orthodontics. Saliva and reflective surfaces, particularly metal brackets, can interfere with light capture and introduce noise into the data. This does not necessarily prevent scanning, but it can reduce accuracy if not managed properly.
Maintaining a dry field and adjusting the scanning angle are simple yet effective ways to improve results. Over time, clinicians develop an instinct for handling these conditions, which significantly improves scan reliability.
Large Crowding Cases
Severe crowding presents one of the most demanding scenarios for digital scanning. Overlapping tooth surfaces and limited visibility make it difficult for the scanner to maintain tracking, increasing the risk of stitching errors.
In these cases, success depends more on scanning technique than on the device itself. A structured path and controlled movement can greatly improve the final model, even in challenging conditions.
Final Summary
An intraoral scanner for orthodontics is not just a digital replacement for traditional impressions it reshapes how orthodontic data is captured, processed, and used throughout treatment. Its value depends less on specifications and more on how well it fits into clinical workflow, operator skill, and treatment focus. When used correctly, it improves consistency, enhances patient experience, and supports more predictable outcomes, making it a practical investment rather than just a technological upgrade.
FAQs
- What is an intraoral scanner used for in orthodontics?
It is used to capture digital full-arch records for aligners, indirect bonding, retainers, treatment planning, and digital model archiving.
- Can intraoral scanning replace traditional impressions?
Yes. In many orthodontic workflows, digital scanning can replace alginate impressions while improving patient comfort and reducing remake risk.
- How accurate are intraoral scanners in orthodontics?
Accuracy varies by device, operator, and clinical conditions, but lab accuracy is often higher than real-world in vivo accuracy.
- Why is full-arch accuracy so important?
Small stitching errors can accumulate across the arch, affecting aligner fit, bracket positioning, occlusion, and long-term treatment planning.
- Which intraoral scanner is best for orthodontists?
The best scanner is the one that fits the clinic’s workflow, case volume, software needs, lab partnerships, and treatment focus.
- Is an open or closed scanner system better?
Open systems offer more flexibility with labs and software, while closed systems often provide smoother integration within a specific treatment ecosystem.
- What makes scanning with brackets challenging?
Metal brackets can create reflection, light scattering, and edge-detection problems, which may reduce scan quality if moisture and angles are not controlled.
- Can an intraoral scanner improve clinic revenue?
Yes. When used consistently, it can support more aligner cases, reduce remakes, improve patient communication, and shorten workflow delays.
- How long does it take to recover the cost of an intraoral scanner?
In a simplified model, a scanner may break even in about 6–10 months, depending on case volume, profit per case, and daily workflow integration.
- What is the most important factor for successful scanner use?
Operator skill and a standardized scan path are critical; even an advanced scanner can produce inconsistent results if used inefficiently.