What Is a Photogrammetry Intraoral Scanner?
A photogrammetry intraoral scanner is a dental scanner designed to capture two different types of information during an implant scan: the surface anatomy of the mouth and the exact 3D position of implant-related markers.
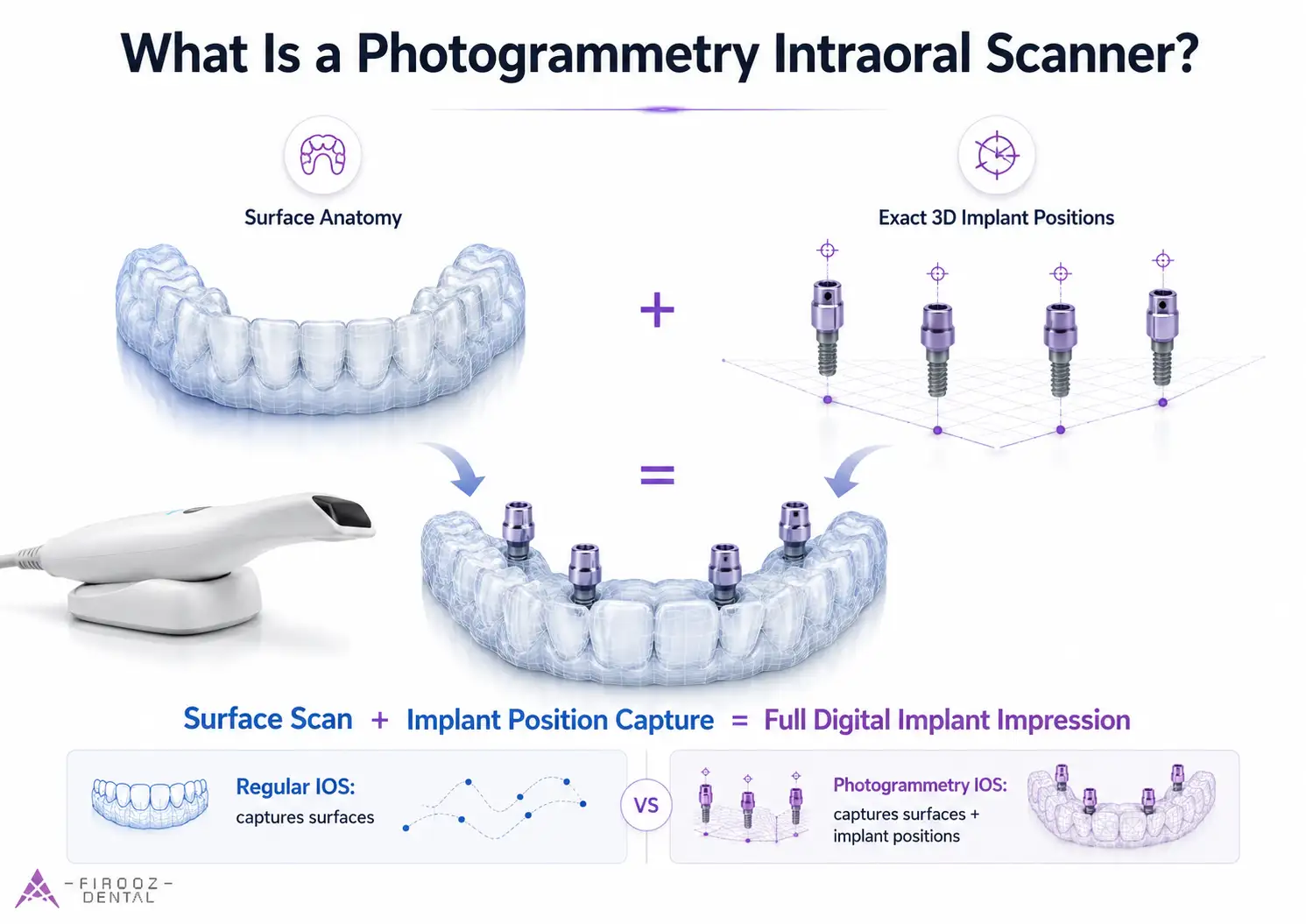
A regular intraoral scanner records shapes: soft tissue, teeth, scan bodies, the arch form, and bite records. That is enough for many single crowns, short-span implant bridges, and routine digital impressions. But in full-arch implant dentistry, the hardest part is not just scanning the gums. The hard part is recording where each implant sits in space and at what angle.
This is where intraoral photogrammetry becomes useful. Instead of depending only on a long surface scan, the scanner reads special markers or coded scan bodies attached to the implants or multi-unit abutments. By recognizing these fixed points from different viewing angles, the system calculates the implant positions more directly.
A simple way to picture it is this:
surface scan + implant position capture = full digital implant impression
The surface scan tells the lab what the mouth looks like. The photogrammetry scan tells the lab where the implants are. Both pieces matter.
What makes it different from a regular intraoral scanner?
The main difference is how implant position is captured.
A regular intraoral scanner builds a 3D model by joining thousands of small images together. This works well when the scanner has enough stable landmarks, such as teeth, clear anatomy, or short scan distances. In a full edentulous arch, those landmarks are limited. The scanner may need to “stitch” a long path across soft tissue, scan bodies, saliva, and moving tissues. Small mismatches can add up.
A photogrammetry IOS is built to reduce that problem by reading implant markers as fixed spatial references. It does not only ask, “What does this surface look like?” It also asks, “Where are these implant connection points in 3D space?”
That does not mean it replaces every other record. Most workflows still need an intraoral surface scan for soft tissue, prosthetic space, bite, and emergence profile. Photogrammetry is best understood as the implant-position part of a digital implant impression, not as the entire clinical record by itself.
here is:
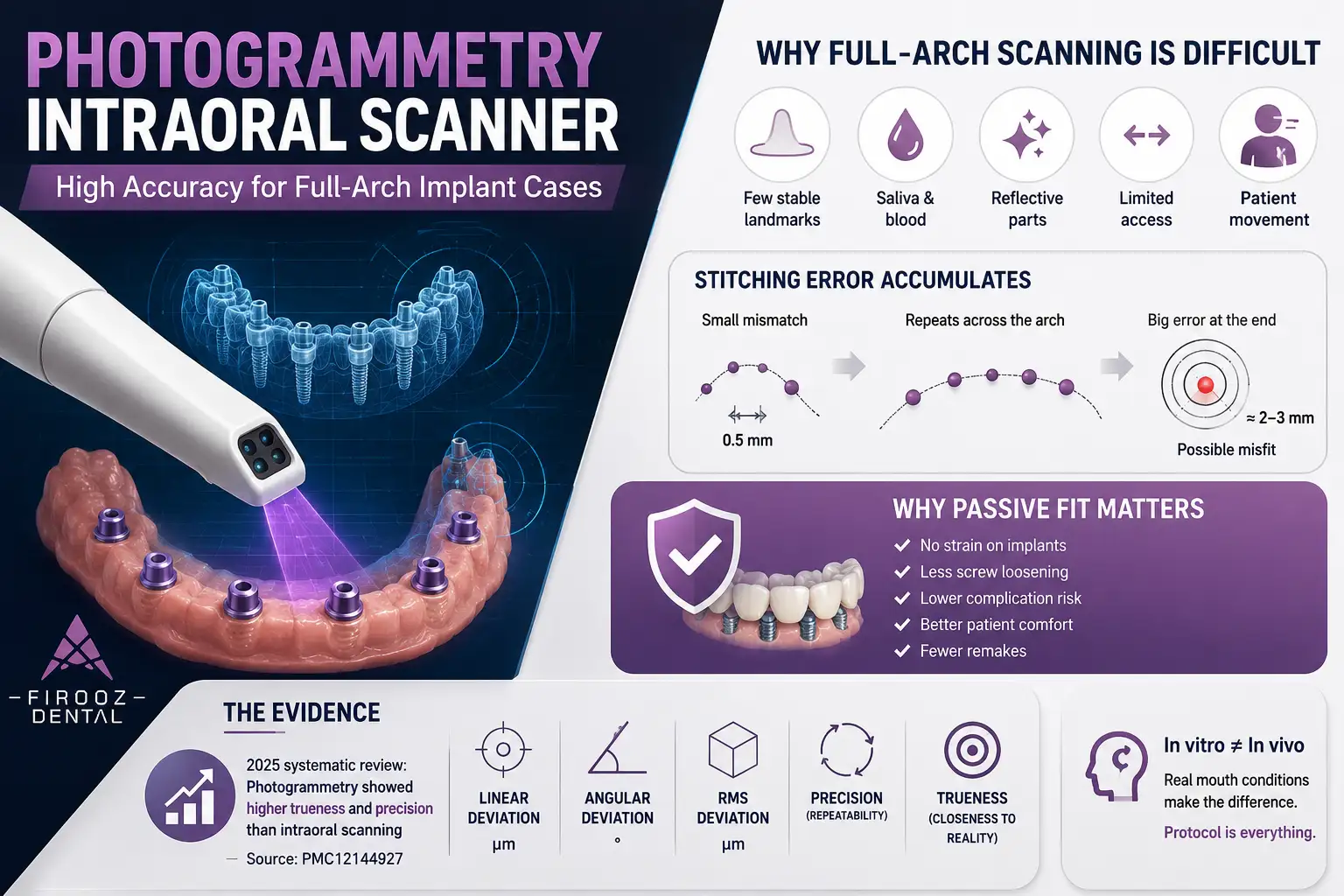
Why Full-Arch Implant Scanning Is So Difficult
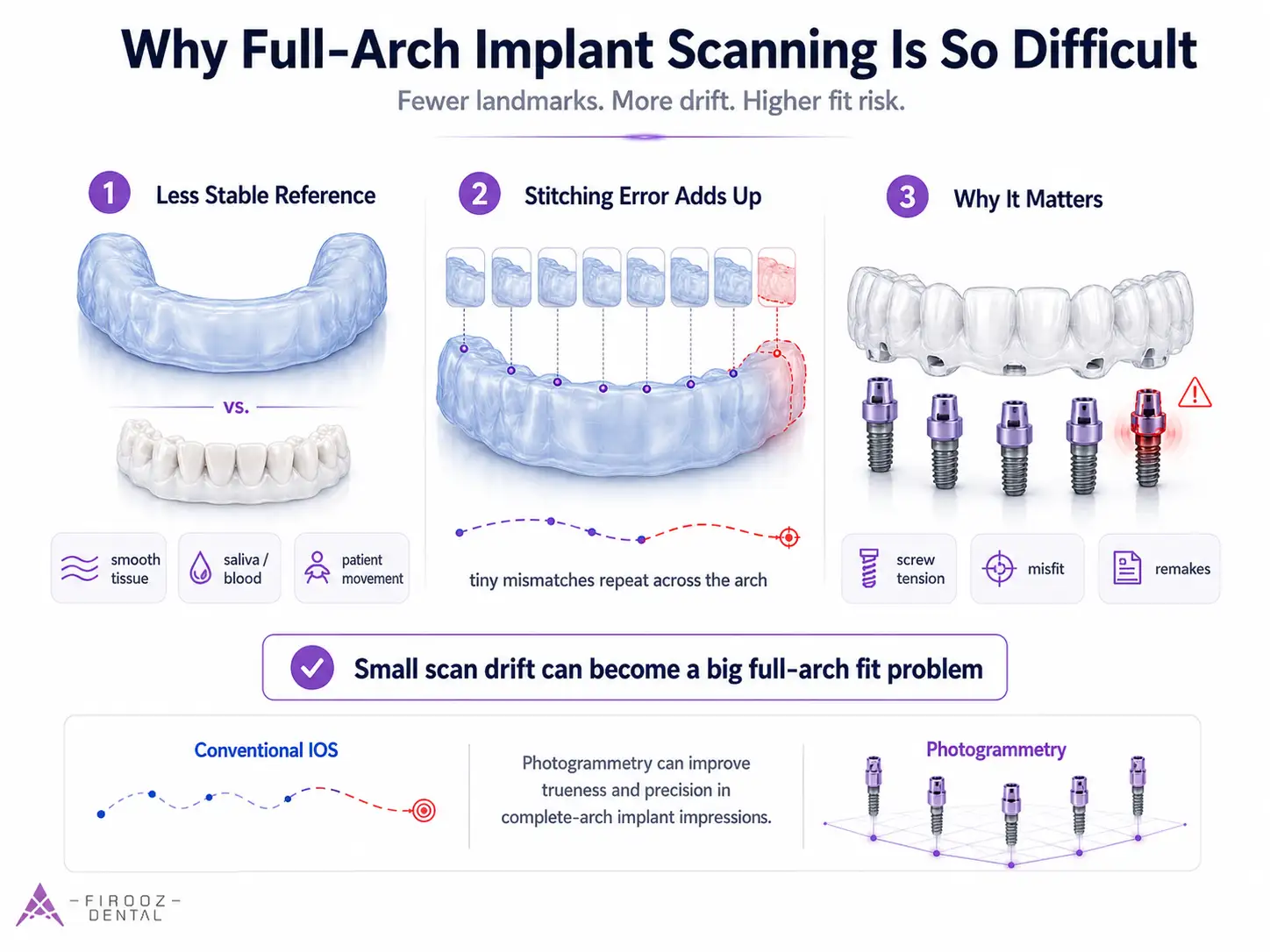
Full-arch implant scanning is difficult because an edentulous arch gives the scanner fewer stable reference points. Natural teeth have edges, cusps, grooves, and hard surfaces that help the scanner track its location. A toothless arch is smoother, softer, wetter, and less distinct.
In real clinical conditions, the scanner also has to deal with saliva, blood, reflective scan bodies, limited access, patient movement, and tissue compression. These factors can make the scan less stable than a clean model scan on a bench.
From practical experience in digital implant workflows, one of the most common mistakes is assuming that a beautiful-looking scan is also an accurate implant record. A scan can look clean on screen and still carry positional error if the scan bodies were not fully seated or if the long-span scan drifted across the arch.
How stitching errors accumulate in conventional IOS scans
Conventional intraoral scanners create a model by joining many small views together. This process is often called stitching. In a short scan, a tiny mismatch may not matter much. In a full arch, the same tiny mismatch can repeat again and again as the scan moves from one side of the mouth to the other.
Think of it like drawing a long line with a ruler that is shifted half a millimeter each time. The first shift may look harmless. After several shifts, the endpoint is no longer where it should be.
That is why IOS stitching error matters so much in full-arch implant scanning. The prosthesis is not supported by flexible teeth. It is connected to implants that are fixed in bone. If the digital model places those implants even slightly away from their true position, the final framework may not seat passively.
Photogrammetry showed higher trueness and precision than intraoral scanning for complete-arch digital implant impressions, although further clinical trials are still needed.
Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC12144927/
Why passive fit matters in All-on-X restorations
Passive fit means the full-arch prosthesis sits on the implants without forcing them into a strained position. In All-on-X and All-on-4 restorations, this is not a small detail. A misfit framework can create screw tension, uneven load, prosthetic complications, screw loosening, material fracture, patient discomfort, or extra lab remakes.
For single implants, minor scan variation may be easier to manage. For a full-arch bridge, all implant positions must work together. Linear deviation and angular deviation both matter. A small angle error at one implant can affect how the framework seats across the entire arch.
This is why a photogrammetry intraoral scanner is mainly discussed in full-arch treatment, not routine single-tooth dentistry.
How Intraoral Photogrammetry Works
Coded scan bodies and reference markers
The workflow starts with special scan bodies. These are not just simple scan posts. They usually include coded patterns, dots, shapes, or horizontal markers that the scanner can recognize. Each marker acts like a known reference point.
The first clinical check is simple but vital: the scan bodies must be fully seated. If one scan body is loose, rotated, contaminated, or placed on the wrong component, the scan may produce bad implant position capture no matter how good the device is.
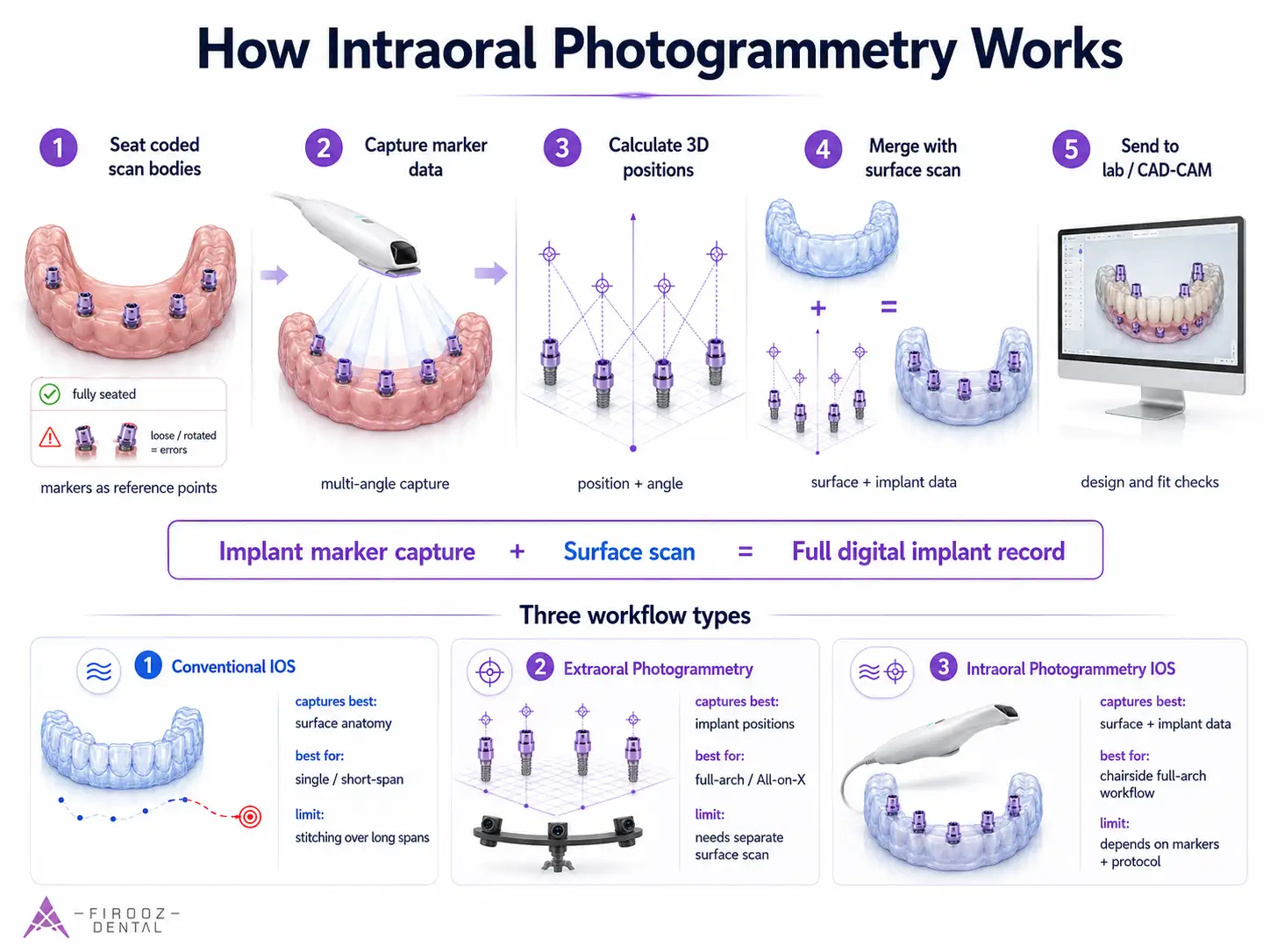
Image capture, triangulation, and spatial calculation
Once the coded scan bodies are in place, the scanner captures them from different angles. The software identifies the visible markers and calculates their positions in 3D space. The principle is similar to locating several fixed points in a room by viewing them from different positions.
This process helps record implant position and angulation without depending only on a long soft-tissue surface scan. For full-arch cases, that is the main value.
Merging photogrammetry data with the intraoral surface scan
After implant positions are captured, the data is combined with the regular intraoral surface scan. The lab then receives both the anatomy and implant coordinates needed for CAD design.
| Step | What happens | Why it matters |
| 1 | Seat coded scan bodies | Wrong seating can distort the whole case |
| 2 | Capture marker data | Records implant position and angle |
| 3 | Scan soft tissue and bite | Adds anatomy, prosthetic space, and occlusion |
| 4 | Merge the records | Combines implant coordinates with surface anatomy |
| 5 | Send to lab for CAD/CAM | Supports full-arch prosthesis design and fit checks |
Photogrammetry IOS vs Conventional IOS vs Extraoral Photogrammetry
Not every digital implant scan uses the same logic. Before choosing a photogrammetry intraoral scanner, it helps to separate three categories: conventional intraoral scanners, dedicated extraoral stereophotogrammetry systems, and built-in intraoral photogrammetry scanners.
Conventional intraoral scanning
Conventional IOS systems such as TRIOS, Primescan, Medit, and iTero are excellent for many daily cases. They record surface anatomy: teeth, soft tissue, scan bodies, bite records, and prosthetic space. For single implants and short-span implant bridges, this is often enough.
The limitation appears in full-arch implant cases. A regular IOS builds the model by joining many small images. When the arch is long, edentulous, wet, or lacks clear landmarks, small stitching errors can add up. This does not mean conventional IOS is poor; it means the case type matters.
Dedicated extraoral stereophotogrammetry systems
Systems such as PIC and ICam4D are designed mainly to record implant positions with very high spatial accuracy. They do this using special markers attached to implants or multi-unit abutments. Their strength is full-arch implant position capture, especially in All-on-X and All-on-4 cases.
Their weakness is that they usually do not replace an intraoral surface scan. You still need soft tissue, occlusion, prosthetic space, and emergence profile records. They may also add cost, extra equipment, and a separate workflow.
Built-in intraoral photogrammetry scanners
This category combines intraoral scanning with photogrammetry-style implant position capture in the same chairside workflow. Devices in this group aim to record surface anatomy and implant marker positions during a single digital process.
The main advantage is convenience: fewer devices, fewer file transfers, and a more direct clinic-to-lab workflow. The main risk is assuming that the scanner alone removes all error. It does not. Scan body seating, marker visibility, software matching, and operator protocol still matter.
| Category | Captures best | Strong cases | Main limits |
| Conventional IOS | Teeth, tissue, scan bodies, bite | Single implants, short-span bridges | Long-span stitching error |
| Extraoral photogrammetry | Implant positions and angulation | Full-arch, All-on-X | Needs extra surface scan |
| Intraoral photogrammetry IOS | Surface scan plus implant marker data | Full-arch chairside workflows | Depends on markers, software, protocol |
What Does the Evidence Say About Accuracy?
Accuracy claims in implant scanning can be confusing because different studies measure different things. A scanner may perform well in one test and less well in another. That is why dentists should look beyond marketing terms and ask: accuracy of what, measured how, and in which clinical setting?
Trueness vs precision: what dentists often confuse
Trueness means how close the scan is to the real implant position. Precision means how repeatable the scanner is when the same object is scanned several times.
A scanner can be precise but not true. In simple words, it may repeat the same error again and again. For full-arch implant work, both matter. You need repeated scans to be consistent, but you also need the digital implant positions to match the patient’s mouth.
Linear deviation, angular deviation, and RMS values
In full-arch implant scans, researchers often measure linear deviation, angular deviation, and RMS deviation.
| Term | Plain meaning | Why it matters |
| Linear deviation | Position error in microns | Affects how the framework seats |
| Angular deviation | Angle error in degrees | Can affect screw channel and fit |
| RMS deviation | Overall 3D difference | Helps compare scan datasets |
| Precision | Repeatability | Shows scan consistency |
| Trueness | Closeness to reality | Shows clinical accuracy |
A 2025 systematic review comparing photogrammetry and IOS in complete-arch digital implant impressions reported better trueness and precision for stereophotogrammetry in most included studies. Some reported ranges also showed lower surface and angular deviations for photogrammetry than IOS.
Photogrammetry showed higher trueness and precision than intraoral scanning for complete-arch digital implant impressions, although further clinical trials are still needed.
Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC12144927/
At the same time, not every study gives the same winner. Some in vitro comparisons show modern IOS devices performing very close to photogrammetry systems, especially when scan conditions are controlled. The practical lesson is simple: photogrammetry scanner accuracy is case-dependent.
Why in vitro results do not always equal chairside performance
Bench tests are useful, but they do not fully copy the mouth. In a real full-arch case, you deal with saliva, blood, cheeks, tongue, limited space, reflective parts, tissue movement, and patient fatigue. A scanner that performs well on a clean model still needs a careful clinical protocol.
Clinical Workflow
A typical full-arch digital workflow starts with the prosthetic plan, not the scanner. The dentist confirms implant stability, multi-unit abutment connection, scan body selection, and tissue condition.
Chairside steps usually include seating the coded scan bodies, checking them visually and radiographically when needed, capturing photogrammetry data, scanning soft tissue, recording bite, and reviewing the files before sending them to the lab.
Before sending the case, check these six items: scan bodies fully seated, correct scan body library, visible marker surfaces, clean tissue scan, usable bite record, and no warning during data matching.
Lab-side steps for CAD/CAM design
The lab receives the implant position file and the surface scan. The technician matches the implant data with the correct digital library, designs the prototype or framework, checks screw access, verifies tissue space, and plans the material.
For a full-arch zirconia or titanium framework, the lab may request a printed model, verification record, or prototype try-in depending on risk level.
Where verification still matters
A photogrammetry intraoral scanner can reduce risk, but it should not remove clinical judgment. For high-value full-arch cases, immediate-load cases, patients with difficult access, or unclear scan body seating, a prototype try-in or passive fit check may still be wise.
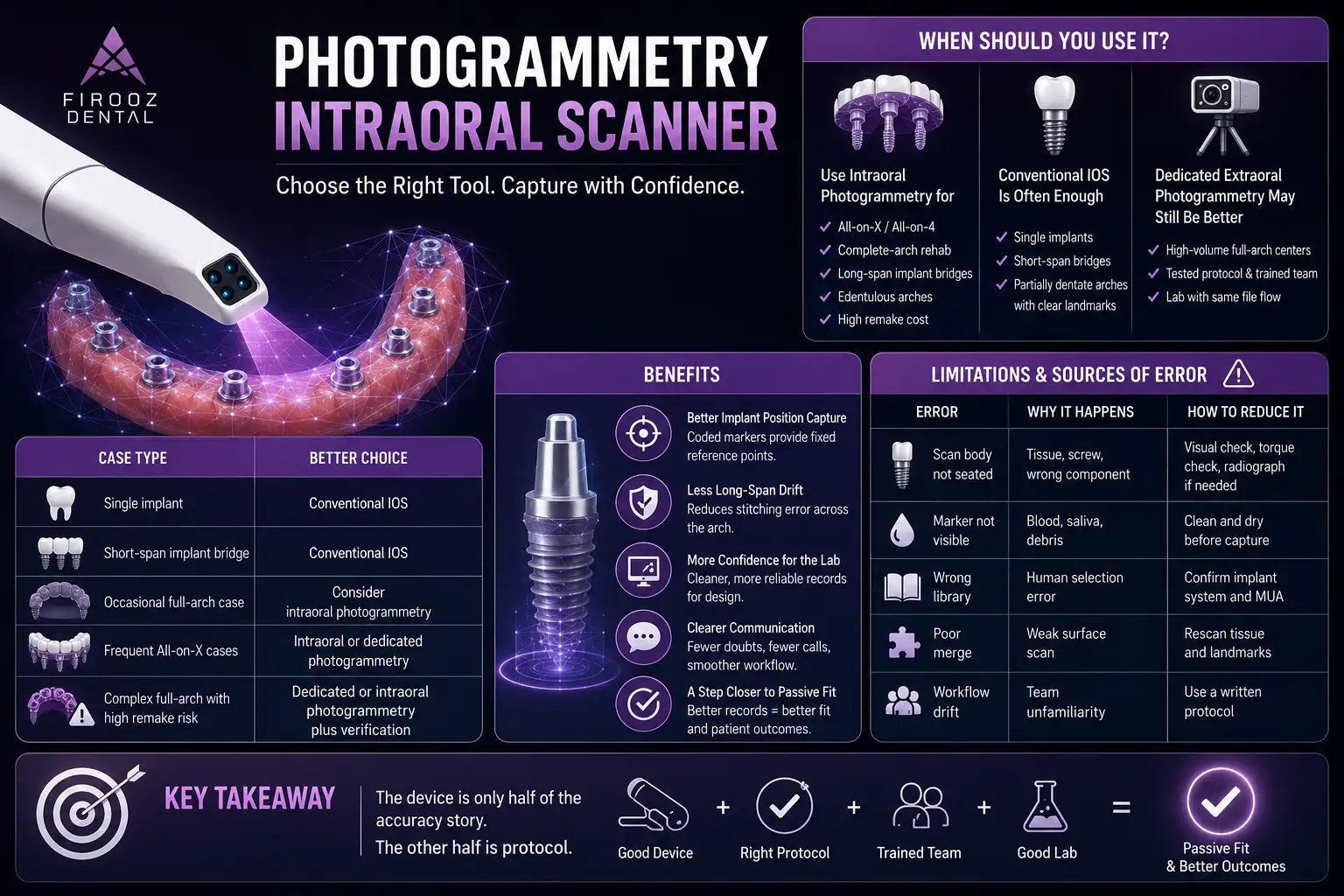
When Should You Use a Photogrammetry Intraoral Scanner?
Consider intraoral photogrammetry for All-on-X, All-on-4, complete-arch implant rehabilitation, long-span implant bridges, edentulous arches, and cases where remake cost is high.
Cases where conventional IOS may be enough
For single implants, short-span bridges, and partially dentate arches with clear landmarks, a conventional IOS may be simpler, cheaper, and fully adequate.
Cases where dedicated extraoral photogrammetry may still be better
High-volume full-arch centers may still prefer dedicated systems when their team already has a tested protocol, trained staff, and a lab that works with the same file flow.
| Case type | Better choice |
| Single implant | Conventional IOS |
| Short-span implant bridge | Conventional IOS |
| Occasional full-arch case | Consider intraoral photogrammetry |
| Frequent All-on-X cases | Intraoral or dedicated photogrammetry |
| Complex full-arch with high remake risk | Dedicated or intraoral photogrammetry plus verification |
Benefits of Photogrammetry Intraoral Scanners
The main benefit is better implant position capture in full-arch cases. Instead of depending only on surface stitching across the whole arch, the scanner reads coded markers that act as fixed reference points.
This can reduce the chance of long-span drift, help the lab design with more confidence, and make clinic-to-lab communication cleaner. It can also help the dentist decide earlier whether a record is usable.
In daily practice, this means fewer doubts before sending the case, fewer calls from the lab about scan body mismatch, and a clearer path toward passive fit. The benefit is not magic; it comes from better records and a tighter protocol.
Limitations and Sources of Error You Should Not Ignore
A photogrammetry IOS can still fail. The most common risk is scan body seating error. If the scan body is not fully seated, the digital implant position is wrong from the start.
Blood, saliva, debris, reflection, and marker damage can also affect recognition. Software matching errors may occur if the wrong library is selected or if the photogrammetry data and surface scan do not match well.
| Error | Why it happens | How to reduce it |
| Scan body not seated | Tissue, screw, wrong component | Visual check, torque check, radiograph if needed |
| Marker not visible | Blood, saliva, debris | Clean and dry before capture |
| Wrong library | Human selection error | Confirm implant system and MUA |
| Poor merge | Weak surface scan | Rescan tissue and landmarks |
| Workflow drift | Team unfamiliarity | Use a written protocol |
In full-arch workflow, the device is only half of the accuracy story. The other half is protocol.
Does Photogrammetry Capture Soft Tissue and Bite?
Photogrammetry captures implant position and angulation. That is its main role.
What still requires an intraoral surface scan
Soft tissue, bite, opposing arch, prosthetic space, emergence profile, and denture contours still need surface scanning or extra records.
| Record | Best captured by |
| Implant position | Photogrammetry |
| Soft tissue | IOS |
| Bite | IOS or bite record |
| Opposing arch | IOS |
| Prosthetic space | IOS plus clinical photos |
Photogrammetry Intraoral Scanner Cost and ROI Considerations
The cost is not only the scanner. Add scan bodies, kits, software fees, training, maintenance, and lab compatibility.
ROI depends on case mix. A clinic doing one full-arch case every few months has a different calculation from a center doing several All-on-X cases weekly.
Before buying, test the scanner on a full-arch model and one real case. Send the files to your own lab and ask whether the workflow reduces remakes, chair time, and design uncertainty.
How to Choose the Right Photogrammetry Intraoral Scanner
Look for published accuracy data, independent studies, implant system compatibility, clean export options, scan body sterilization rules, lab acceptance, training quality, and support after purchase.
Questions to ask before buying: Which implant systems are supported? Are the scan bodies autoclavable? What files can be exported? Does my lab accept this workflow? Is there clinical evidence, not only brand claims?
Is a Photogrammetry Intraoral Scanner Worth It?
Use it if full-arch implant work is a regular part of your practice. You may not need it if your work is mostly single implants and short spans. Test it before buying if your lab, team, or implant systems may limit the workflow.
FAQs
- What is a photogrammetry intraoral scanner used for?
A photogrammetry intraoral scanner is mainly used to capture implant positions in full-arch cases such as All-on-X and All-on-4 treatments. It helps record the 3D position and angle of implants more directly than a regular surface scan, especially when the arch has few natural landmarks.
- Is intraoral photogrammetry better than a regular intraoral scanner?
Not always. A regular intraoral scanner is often enough for single implants, short-span bridges, and partially dentate cases. Intraoral photogrammetry becomes more useful in full-arch implant cases, where long-span stitching errors can affect the final fit of the prosthesis.
- Does a photogrammetry intraoral scanner capture soft tissue?
Photogrammetry mainly captures implant position and angulation. Soft tissue, bite, opposing arch, prosthetic space, and emergence profile usually still need a regular intraoral surface scan or other clinical records.
- Do I still need scan bodies with intraoral photogrammetry?
Yes. Most photogrammetry IOS workflows use coded scan bodies or markers attached to implants or multi-unit abutments. These markers help the scanner calculate the exact implant positions. If a scan body is not fully seated or is covered by blood or saliva, the result can be inaccurate.
- Is a photogrammetry intraoral scanner necessary for All-on-X cases?
It is not mandatory, but it can be very useful. All-on-X cases need accurate implant position capture to support passive fit. If your clinic regularly handles full-arch implant restorations, a photogrammetry intraoral scanner may reduce scan uncertainty and remake risk.
- What can cause errors in intraoral photogrammetry scans?
Common causes include poor scan body seating, wrong implant library selection, blood or saliva covering coded markers, reflective surfaces, poor surface scan quality, and incorrect data matching between the photogrammetry file and the intraoral scan.
- How should I choose a photogrammetry intraoral scanner?
Look at accuracy evidence, implant system compatibility, scan body design, sterilization rules, software workflow, lab acceptance, file export options, training quality, and total cost. Before buying, test the scanner on a full-arch model and ask your own lab to review the files.