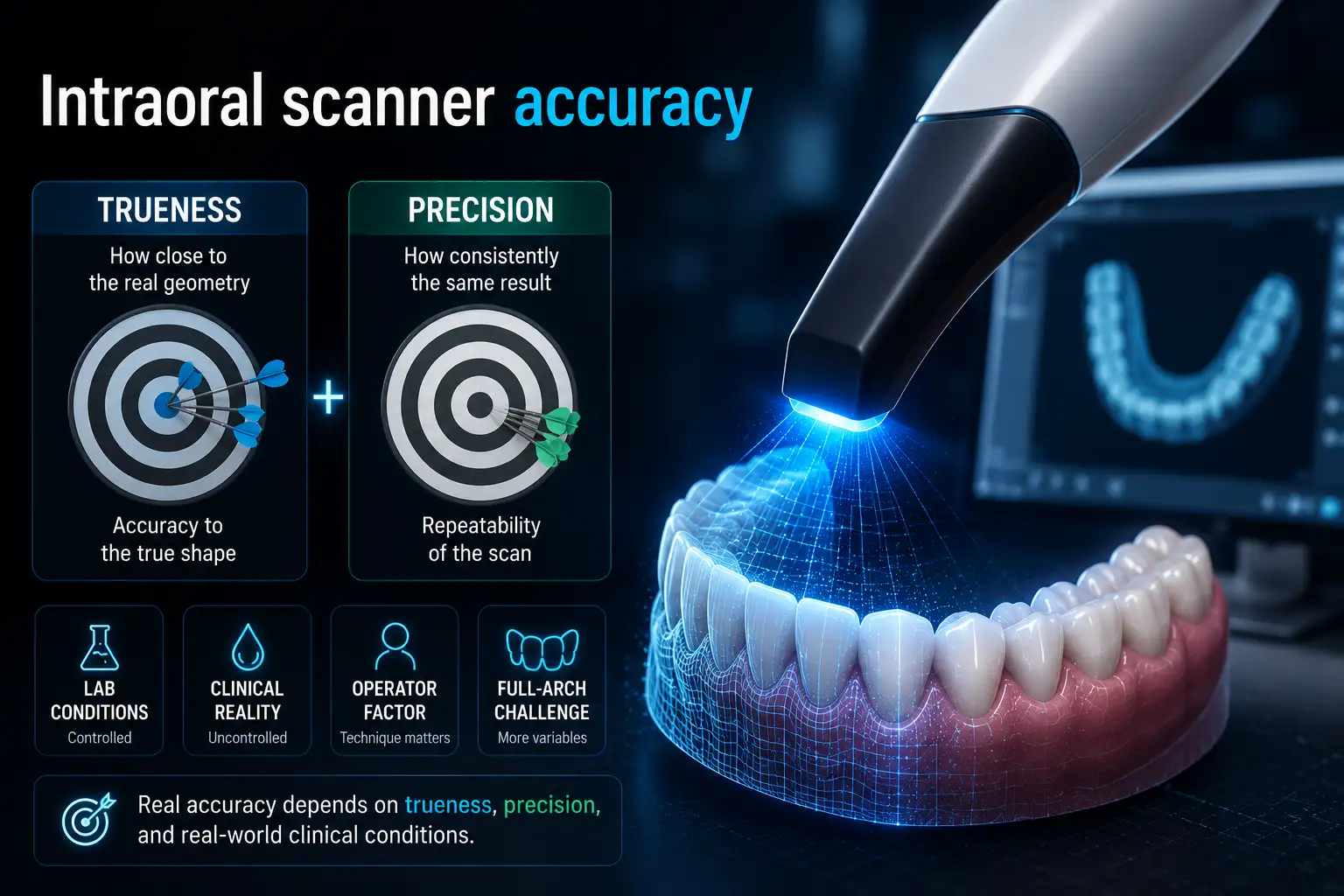
Intraoral scanner accuracy is not just the micron number shown in a brochure; it means how closely and consistently a scanner captures the real shape of teeth, soft tissue, margins, or scan bodies in actual clinical conditions. In practice, accuracy depends on both trueness how close the scan is to reality and precision how repeatable the scan is. An intraoral scanner may perform well in laboratory tests but lose accuracy in the mouth because of saliva, blood, limited access, patient movement, reflective surfaces, or long-span scans. That is why digital impression accuracy must be judged by clinical indication, not marketing numbers alone.
The accuracy of a digital impression affects the final fit of every restoration. Even a small scanning error can lead to open margins, occlusal discrepancies, poor proximal contacts, or internal misfit. In implant dentistry, the risk is higher because implants cannot compensate for minor errors like natural teeth.
As the scan area becomes larger, accuracy becomes harder to maintain. A single crown may tolerate small deviations, but long-span bridges and full-arch implant cases are much less forgiving. During longer scans, stitching errors can accumulate, especially in posterior areas where access and visibility are limited.
Poor scan accuracy can increase chair time, laboratory costs, rescans, adjustments, and remake risk. A more accurate STL file improves communication between the clinic and laboratory and supports a better CAD/CAM workflow.
| Clinical Outcome | Effect of Poor Scan Accuracy |
| Marginal fit | Open margins |
| Occlusion | Bite discrepancies |
| Implant prosthesis | Passive fit problems |
| Long-span restorations | Framework misfit |
| Chairside workflow | More adjustments |
| Laboratory workflow | Higher remake risk |
For this reason, intraoral scanner accuracy should not be judged only by advertised micron values. The key question is whether the scanner can maintain clinically acceptable accuracy in real restorative workflows, especially full-arch and implant-supported cases.
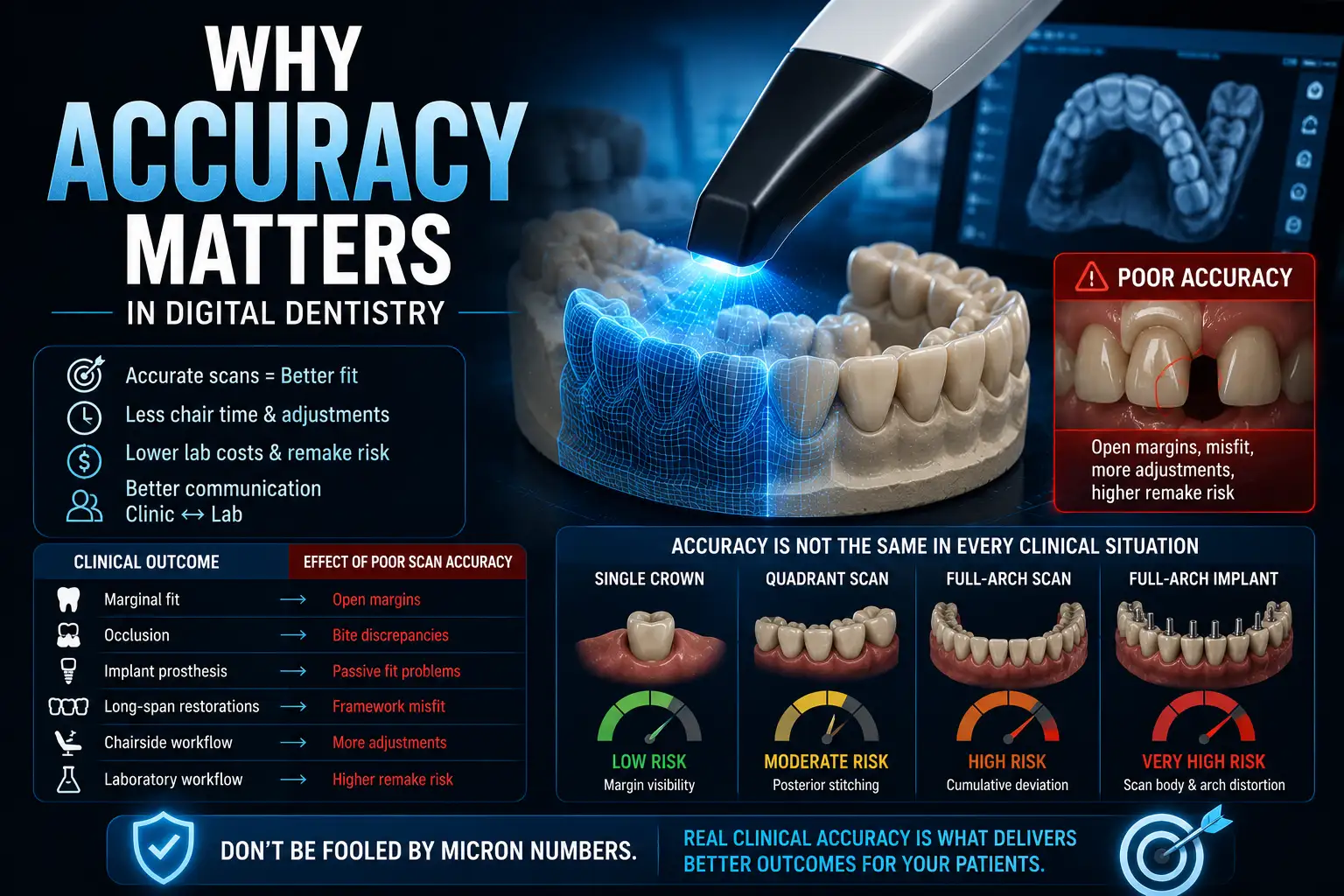
Intraoral scanner accuracy changes with the clinical indication. A scanner may perform very well for a single crown but show greater deviation in full-arch or implant cases because longer scans create more stitching errors.
Single crowns and quadrant scans are usually more predictable because the scanned area is limited. Full-arch scans are more demanding, and full-arch implant cases are the most technique-sensitive because scan bodies provide fewer anatomical reference points than natural teeth.
| Clinical Scenario | Accuracy Risk | Main Error Source |
| Single crown | Low | Margin visibility |
| Quadrant scan | Moderate | Posterior stitching |
| Full-arch scan | High | Cumulative deviation |
| Full-arch implant | Very high | Scan body and arch distortion |
This is why scanner accuracy should be judged by clinical use, not by one micron value. Short-span accuracy does not automatically mean strong full-arch performance.
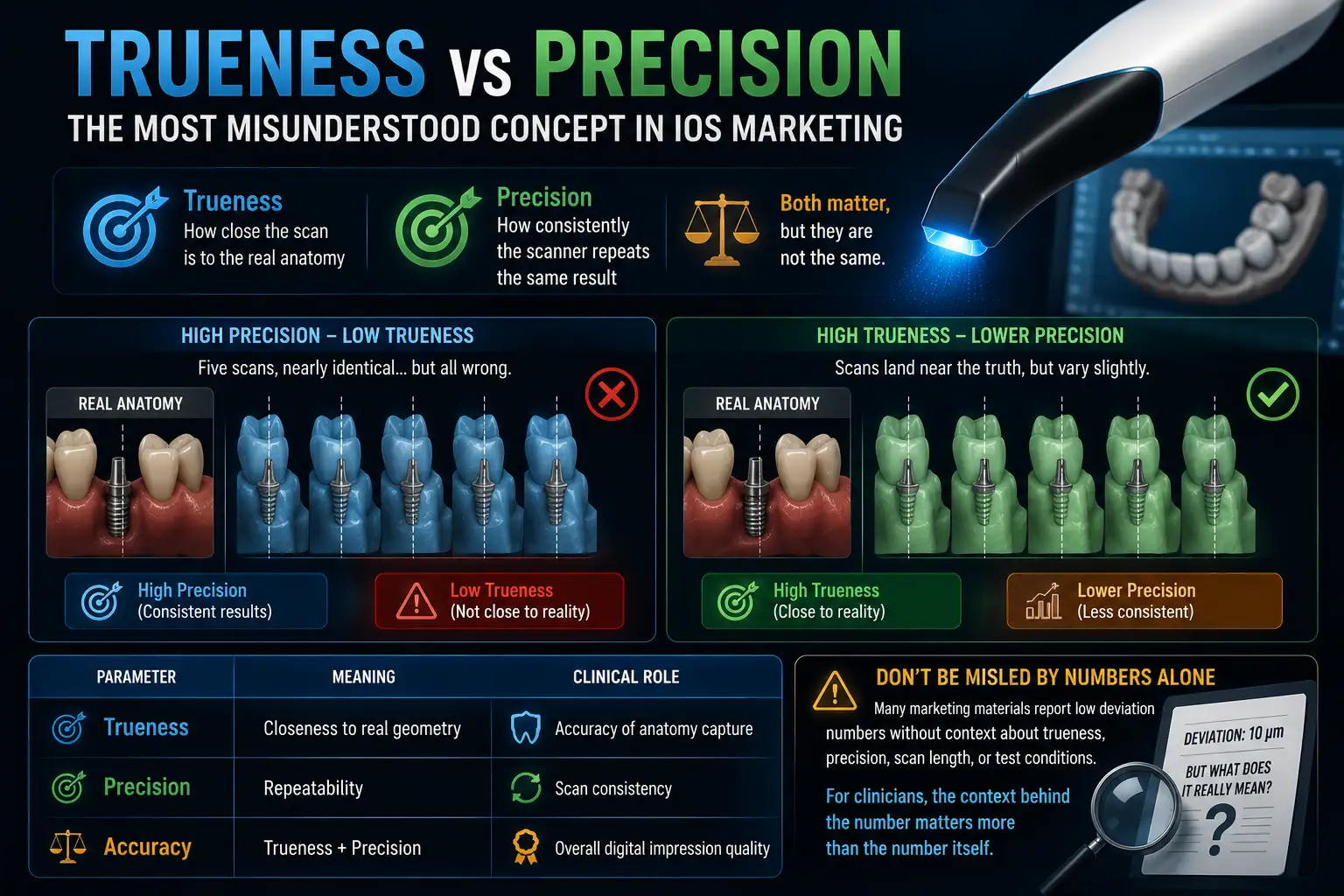
Trueness means how close the scan is to the real anatomy. Precision means how consistently the scanner repeats the same result. Both matter, but they are not the same.
A scanner can be precise but still inaccurate. For example, if five scans produce nearly identical STL files but all show the distal implant in the wrong position, precision is high while trueness is poor.
| Parameter | Meaning | Clinical Role |
| Trueness | Closeness to real geometry | Accuracy of anatomy capture |
| Precision | Repeatability | Scan consistency |
| Accuracy | Trueness + precision | Overall digital impression quality |
Many marketing materials report low deviation numbers without explaining whether they refer to trueness, precision, scan length, or test conditions. For clinicians, the context behind the number matters more than the number alone.
An intraoral scanner does not capture the mouth in one image. It records thousands of small images or video frames and combines them into a 3D model. The final STL file depends on image matching, stitching, and software reconstruction.
Different scanners use different optical methods:
The scan path also affects accuracy. Abrupt movement, saliva, reflective surfaces, missing data, or scan interruption can reduce STL quality. In implant cases, this is harder because scan bodies offer fewer natural landmarks than teeth.
| Workflow Step | Main Function | Possible Error |
| Image acquisition | Surface capture | Reflection, saliva, movement |
| Image stitching | Merging scan frames | Cumulative deviation |
| Surface reconstruction | Building 3D geometry | Missing data |
| STL generation | Exporting the model | Smoothing or distortion |
Scanner performance depends on both hardware and software. Two scanners with similar optics may produce different results because their reconstruction algorithms process scan data differently.
Several clinical and technical factors can reduce intraoral scanner accuracy, even when the device performs well in lab tests. These issues become more important in long-span and implant-supported workflows.
Saliva, blood, and reflective surfaces interfere with optical capture and may cause missing data around margins or scan bodies. Limited posterior access, patient movement, and soft tissue interference can also interrupt image stitching and distort the STL file.
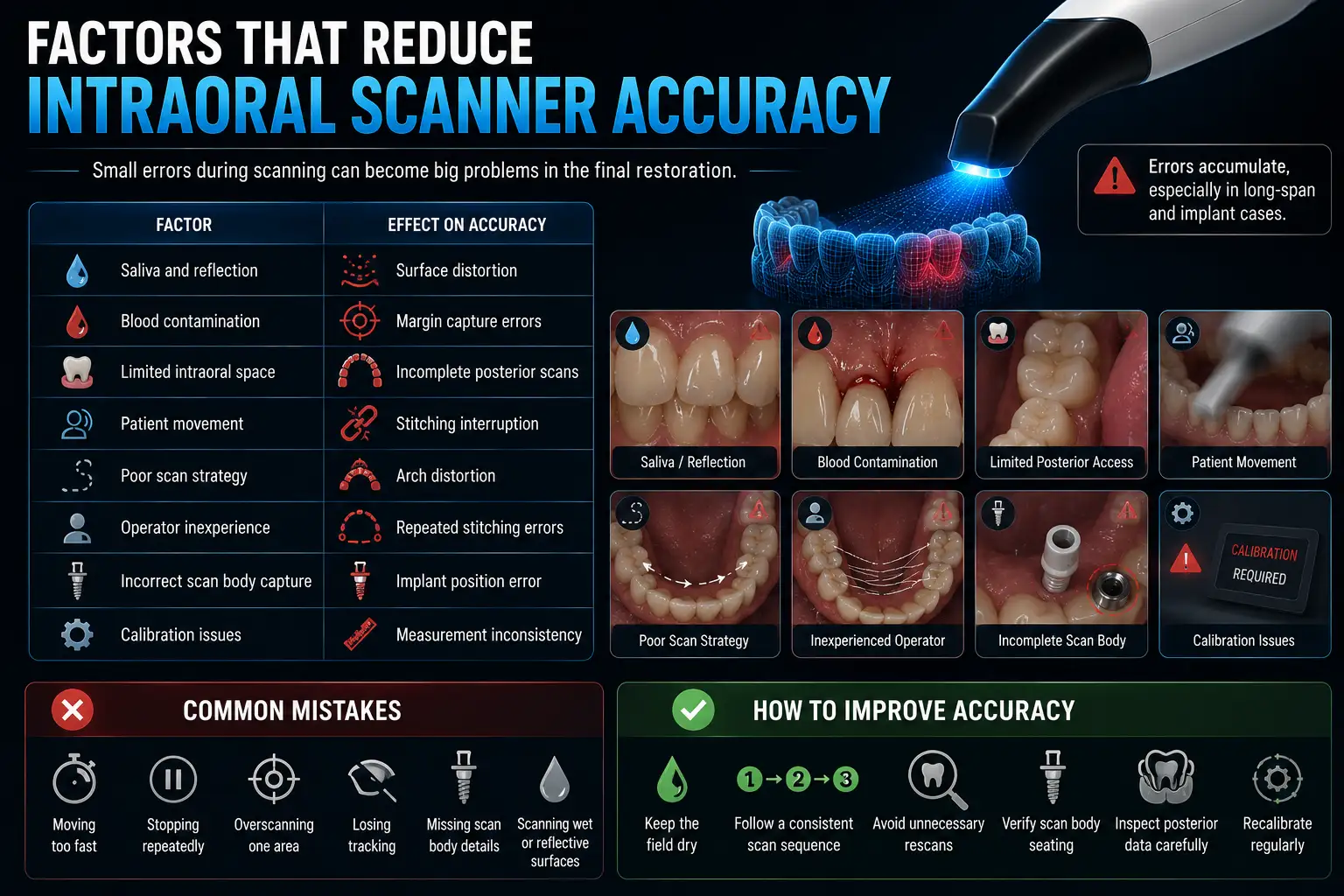
Operator technique is another major factor. A smooth, continuous scan path usually produces better results than repeated stops, sudden movements, or excessive rescanning. In implant cases, incomplete scan body capture can directly affect prosthetic fit.
| Factor | Effect on Accuracy |
| Saliva and reflection | Surface distortion |
| Blood contamination | Margin capture errors |
| Limited intraoral space | Incomplete posterior scans |
| Patient movement | Stitching interruption |
| Poor scan strategy | Arch distortion |
| Operator inexperience | Repeated stitching errors |
| Incorrect scan body capture | Implant position error |
| Calibration issues | Measurement inconsistency |
Common mistakes include moving too fast, stopping repeatedly, overscanning one area, losing tracking, missing scan body details, and scanning wet or reflective surfaces without proper isolation.
To improve accuracy, keep the field dry, follow a consistent scan sequence, avoid unnecessary rescans, verify scan body seating, inspect posterior data, and recalibrate the scanner regularly.
Full arch scan accuracy is difficult because the software must merge many overlapping images into one continuous model. Each overlap can add a small deviation, and these deviations may accumulate across the arch.
Distortion often appears in posterior areas where access, visibility, and reference points are weaker. In dentate arches, natural tooth anatomy helps the software track position. In full-arch implant cases, scan bodies provide fewer geometric references, making tracking less stable.
| Workflow Type | Main Accuracy Challenge |
| Single crown | Margin capture |
| Quadrant scan | Local stitching error |
| Full-arch dentate scan | Arch distortion |
| Full-arch implant scan | Implant position and passive fit error |
Digital impressions usually perform well for short-span restorations, but complete-arch workflows remain more technique-sensitive. Some conventional impressions may still provide more consistent results in certain full-arch implant cases.
Implant cases are more sensitive to scan errors because implants do not have the natural mobility of teeth. Small inaccuracies can transfer stress to screws, implants, and prosthetic frameworks.
The scan body is one of the most important variables. It tells the software the implant position and angulation. If it is not captured fully, the prosthetic position may be inaccurate. Implant angulation, tissue depth, interimplant distance, and posterior access also affect scan quality.
| Implant Variable | Effect on Accuracy |
| Scan body geometry | Defines positional reference |
| Implant angulation | Affects stitching consistency |
| Tissue depth | Reduces visibility |
| Interimplant distance | Increases deviation risk |
| Posterior position | Limits scanner access |
Passive fit is essential in implant prosthodontics. In full-arch cases, small scan errors can accumulate and create framework tension, even when each individual deviation seems minor.
Many scanner brochures advertise very low micron values, but those numbers often come from controlled lab conditions. Real clinical scanning includes saliva, blood, patient movement, limited access, soft tissue interference, and reflective materials.
| Laboratory Environment | Real Clinical Environment |
| Dry surfaces | Saliva and moisture |
| Stable models | Patient movement |
| Ideal access | Restricted posterior access |
| No soft tissue movement | Tongue and cheek interference |
| Controlled scan path | Operator variability |
Another issue is that manufacturers may report trueness, precision, or average deviation from different test designs. A value measured on a single crown model cannot be compared directly with full-arch implant performance.
For clinicians, the key question is not which scanner shows the lowest lab number, but whether it maintains clinically acceptable accuracy in real restorative workflows.
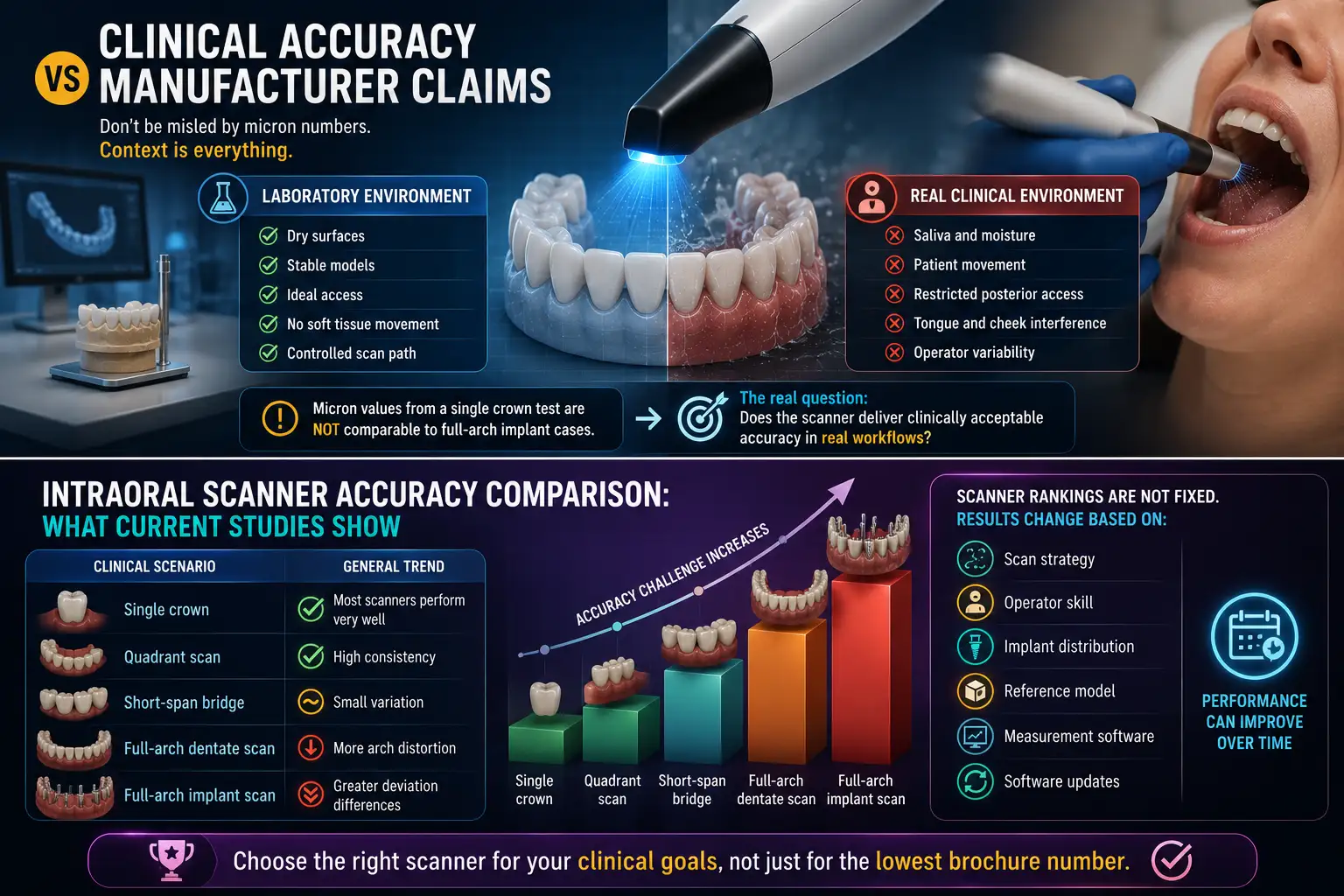
Current research shows that most modern intraoral scanners perform well for single crowns, quadrant scans, and many short-span restorations. Differences become more visible in full-arch and implant-supported cases.
| Clinical Scenario | General Trend |
| Single crown | Most scanners perform very well |
| Quadrant scan | High consistency |
| Short-span bridge | Small variation |
| Full-arch dentate scan | More arch distortion |
| Full-arch implant scan | Greater deviation differences |
Scanner rankings are not fixed. Results change based on scan strategy, operator skill, implant distribution, reference model, and measurement software. Software updates can also change scanner performance over time.
Overall, scanner selection should depend on the intended clinical use, not only brochure values. A scanner suitable for routine crown and bridge cases may not perform the same way in complete-arch implant rehabilitation.
Yes. Operator experience affects scan quality, especially in full-arch and implant cases. Skilled users usually maintain smoother movement, stable overlap, and fewer interruptions. Beginners often move too fast, rotate the scanner excessively, skip landmarks, or stop and restart too often.
| Operator Behavior | Effect on Accuracy |
| Continuous scan path | Better stitching |
| Abrupt movement | More deviation |
| Excessive rescanning | Reconstruction errors |
| Stable overlap | Better tracking |
| Interrupted scanning | Higher distortion |
A stable full-arch scan usually starts from posterior occlusal surfaces, moves continuously across the arch, then captures lingual and buccal surfaces. Missing areas should be corrected carefully, not by repeatedly rescanning large sections.
Improving digital impression accuracy depends on workflow control. Even a strong scanner can produce a distorted STL file if isolation, scan path, or tissue management is poor.
Keep the field dry, manage soft tissue, and avoid saliva pooling around margins or scan bodies. Use a structured scan path with stable overlap, move slowly in posterior areas, and limit rescans to small missing areas. Calibration should also follow the manufacturer’s schedule.
| Clinical Step | Recommendation |
| Moisture control | Keep the field dry |
| Scan path | Use one structured sequence |
| Posterior capture | Move slowly |
| Scan bodies | Confirm full visibility |
| Rescanning | Correct only missing areas |
| Calibration | Recalibrate regularly |
| Soft tissue | Retract before margin capture |
Small improvements in technique often reduce more error than changing the scanner model.
No. Digital impressions are not always more accurate in every situation. The result depends on restoration type, scan length, implant distribution, operator technique, and intraoral conditions.
For single crowns, quadrant scans, and short-span bridges, modern intraoral scanners usually perform very well. They also reduce material distortion, stone expansion errors, and communication delays.
Complete-arch and implant-supported workflows are more complex. In some full-arch implant cases, conventional impressions may still provide more consistent results.
| Workflow | Digital Impression | Conventional Impression |
| Single crown | Excellent | Excellent |
| Quadrant scan | Excellent | Excellent |
| Short-span bridge | Very good | Very good |
| Full-arch dentate | Variable | Stable |
| Full-arch implant | Technique-sensitive | Often more consistent |
The best choice depends on the case. Digital and conventional workflows both have strengths and limitations.
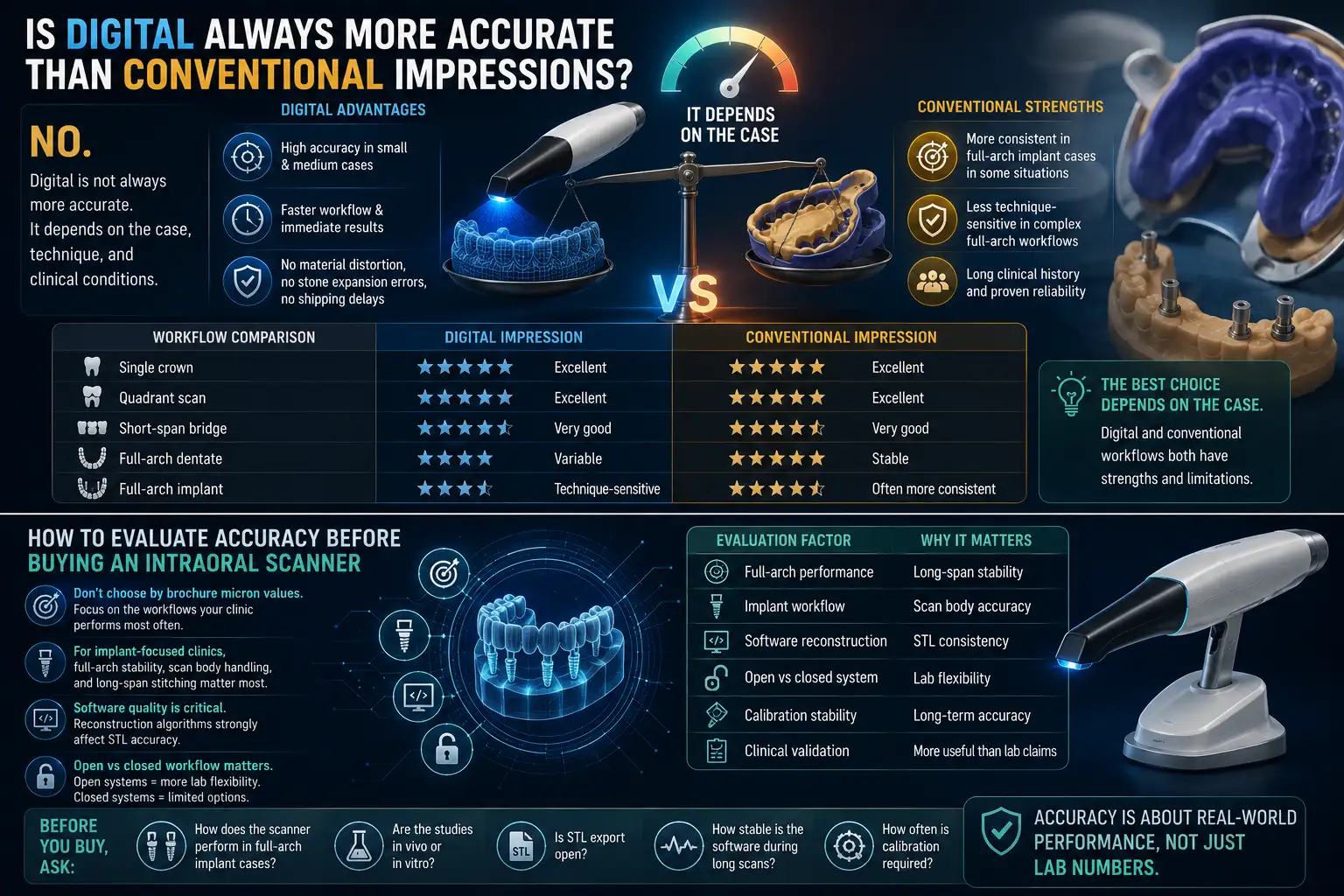
Do not choose an intraoral scanner only by brochure micron values. Accuracy should be judged based on the treatments your clinic performs most often.
For implant-focused clinics, full-arch stability, scan body handling, and long-span stitching behavior matter more than single-crown test results. Software quality is also important because reconstruction algorithms strongly affect STL accuracy.
Open versus closed workflow should also be considered. Open systems usually offer more lab flexibility, while closed systems may limit future options.
| Evaluation Factor | Why It Matters |
| Full-arch performance | Long-span stability |
| Implant workflow | Scan body accuracy |
| Software reconstruction | STL consistency |
| Open vs closed system | Lab flexibility |
| Calibration stability | Long-term accuracy |
| Clinical validation | More useful than lab claims |
Before purchasing, ask how the scanner performs in full-arch implant cases, whether studies are in vivo or in vitro, whether STL export is open, how stable the software is during long scans, and how often calibration is needed.
Intraoral scanner accuracy should not be judged only by brochure specifications. Real accuracy depends on scan strategy, operator experience, software reconstruction, scan length, moisture control, tissue management, and implant complexity.
Modern intraoral scanners perform very well in single crowns, quadrant scans, and short-span workflows. Full-arch and implant-supported cases remain more demanding because stitching deviation can accumulate across the arch.
Digital impressions are not always superior to conventional impressions in every indication. The better choice depends on the restorative goal, clinical environment, and workflow.
For dentists and laboratories, the main question is not which scanner advertises the lowest micron value, but which system maintains clinically acceptable accuracy in real practice.
Clinically acceptable accuracy depends on the indication. Single crowns tolerate small deviations, while full-arch implant restorations require much higher accuracy and passive fit stability.
Neither is more important alone. A clinically reliable scan requires both high trueness and high precision to reproduce anatomy accurately and consistently.
Full-arch scans contain thousands of stitched images. Small stitching deviations accumulate across the arch, especially in posterior regions.
Yes. Saliva and reflective surfaces interfere with optical capture and may create missing data or distorted margins during scanning.
Yes for many cases, but implant workflows are more technique-sensitive because scan body capture and stitching stability directly affect prosthetic fit.
Many advertised values come from controlled laboratory studies that do not reflect real intraoral conditions such as movement, moisture, or limited access.
Yes. Experienced operators usually maintain more stable scan paths, reduce tracking loss, and create fewer stitching errors during long scans.
Not always. Digital impressions perform very well in many restorative cases, but some full-arch implant workflows may still benefit from conventional impressions.
Cumulative stitching deviation is one of the main causes of distortion in complete-arch digital impressions.
Dentists should evaluate full-arch performance, implant workflow quality, software reconstruction, STL export flexibility, calibration stability, and clinical evidence instead of brochure values alone.