An intraoral scanner is a dental device used to capture a direct digital impression of the teeth and surrounding oral structures. Instead of relying on physical impression trays and materials, the scanner records a series of optical images inside the mouth and converts them into a precise three-dimensional model. This process is commonly referred to as intraoral scanning, and the result is what dentists call a digital dental impression. The term is accurate because the scan serves the same clinical purpose as a conventional impression: recording tooth position, shape, and spatial relationships for diagnosis, treatment planning, and fabrication of restorations.
Instead of reading the entire article, you can listen to the short podcast below:

From a practical standpoint, intraoral scanning represents a shift from material-based impressions to image-based records. As the scanner is moved over the teeth, it continuously captures surface data, which is processed in real time to build a complete digital model. This model can then be used for crowns, bridges, implants, orthodontic appliances, and other dental procedures. For dental practices in Canada, intraoral scanners are now a routine part of digital workflows, not because they add complexity, but because they reduce retakes, improve communication with dental laboratories, and provide a clear visual reference that both clinicians and patients can easily understand.
what is dental scanner and how it works? see in this video:
Intraoral scanning starts with the direct recording of the visible surfaces of teeth and surrounding soft tissues using an intraoral optical scanner. The scanner projects a controlled light pattern onto the dental structures, while internal sensors measure how that light returns from different surfaces. Because enamel, dentin, gingiva, and restorative materials reflect light in different ways, the scanner is able to distinguish fine surface detail and depth without physical contact or impression material.
As the clinician moves the scanner tip along the dental arch, the device continuously captures surface data. Instead of producing a single image, the scanner collects a large number of closely spaced surface measurements. Each measurement represents a specific point in three-dimensional space. Together, these points form the foundation of the digital impression.
From a clinical perspective, the scanning process typically follows a structured sequence:
This method allows the scanner to build a complete surface record while minimizing missed areas. Because no trays or impression materials are involved, patient discomfort is reduced, and the risk of distortion caused by material shrinkage or movement is eliminated. For most patients, the process feels similar to having an intraoral camera used, rather than a conventional impression taken.
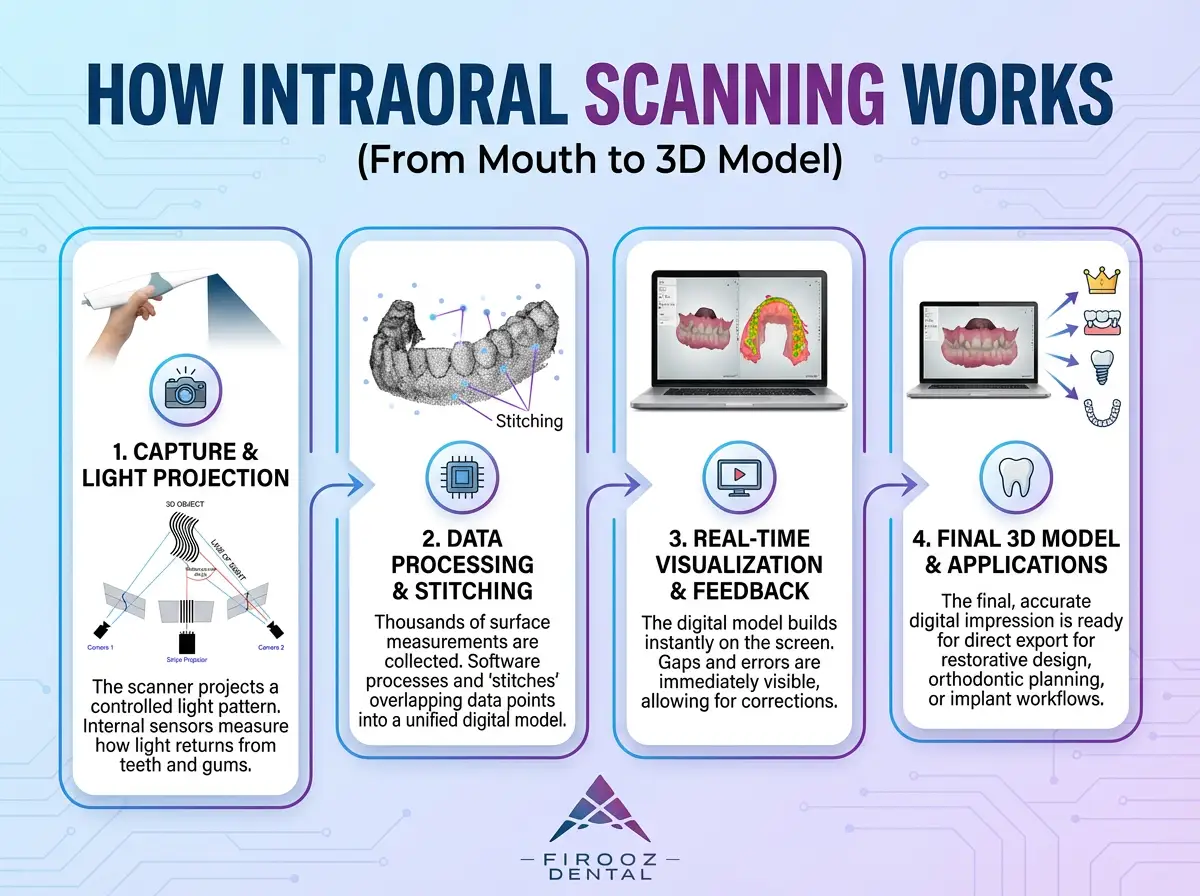
Once surface data is collected, the scanner’s software processes the information by comparing each new data segment with previously captured areas. This comparison allows the system to determine how individual surface sections relate to one another spatially. The process is commonly known as stitching, but in practical terms, it is a continuous alignment of overlapping surface data to form a single digital model.
The quality of this stage depends heavily on scanning technique. Consistent movement and sufficient overlap between scanned areas help the software maintain accurate alignment. Irregular motion or skipped regions can result in incomplete or distorted areas of the model.
During scanning, the clinician sees the digital model forming on the screen in real time. This visual feedback serves several practical purposes:
Common factors that affect scan quality include moisture control, patient movement, reflective surfaces, and scanning speed. In everyday clinical use, proper isolation and a steady scanning path are among the most important contributors to reliable results. When these conditions are met, the final output is a complete three-dimensional digital model of the dentition.
This digital model can then be exported directly for restorative design, orthodontic planning, or implant workflows. Because the information is already in digital form, it can be shared with dental laboratories or planning software without additional conversion steps, remakes, or physical shipping.

Modern intraoral scanners rely on different optical principles to record the shape of teeth and soft tissues. These systems were developed to solve the same clinical task capturing an accurate digital impression but they approach the problem in different ways. Understanding these technologies helps clinicians interpret scan results more realistically and recognize why scanners may behave differently in certain clinical situations.
Rather than focusing on technical specifications, it is more useful to understand how each technology interacts with tooth surfaces, moisture, and scanning technique at the chairside.
Most intraoral scanners used in dental practices today rely on optical scanning methods. These systems capture surface geometry by projecting light onto teeth and recording how that light returns to the scanner’s sensors. The differences between technologies lie in how depth information is calculated and how surface data is assembled.
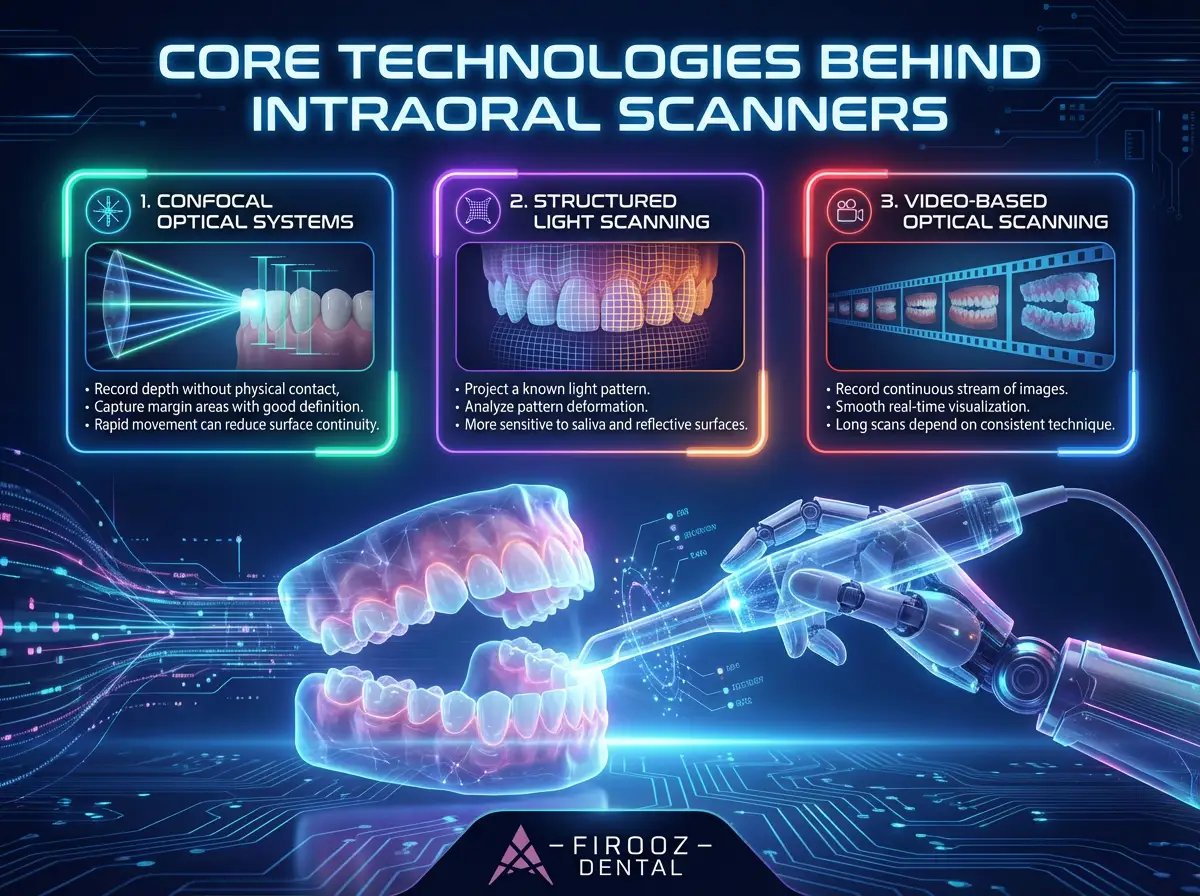
Confocal scanning works by capturing images at multiple focal depths. Instead of relying on a single distance measurement, the system evaluates which surface points appear in focus at different depths and uses this information to calculate surface position.
From a clinical perspective, confocal systems are designed to:
However, scanning technique still matters. Rapid movement or poor overlap between passes can reduce surface continuity, especially in larger spans.
Structured light scanners project a known light pattern often a grid or stripe onto the teeth. The scanner then analyzes how that pattern deforms when it hits curved surfaces. By measuring this deformation, the system calculates the three-dimensional shape of the dentition.
Clinically, structured light systems tend to:
Proper moisture control plays a major role in maintaining reliable surface capture with this approach.
Video-based scanners record a continuous stream of images as the scanner moves through the mouth. Instead of capturing isolated frames, the system processes many images per second and builds the digital model progressively.
This method offers practical advantages:
At the same time, long scans depend heavily on consistent technique, since accumulated alignment errors can affect full-arch results.
If you want to know more but briefly about intraoral scanners, don’t mist this:
The term “laser scanner” is often misunderstood in dentistry. In the context of intraoral scanning, laser refers only to a controlled light source used for surface measurement. It does not involve heat, cutting, or tissue interaction.
What Laser Means in Dental Scanning
In laser-based intraoral scanners:
The energy levels involved are safe for intraoral use and are comparable to other dental optical devices already used in daily practice.
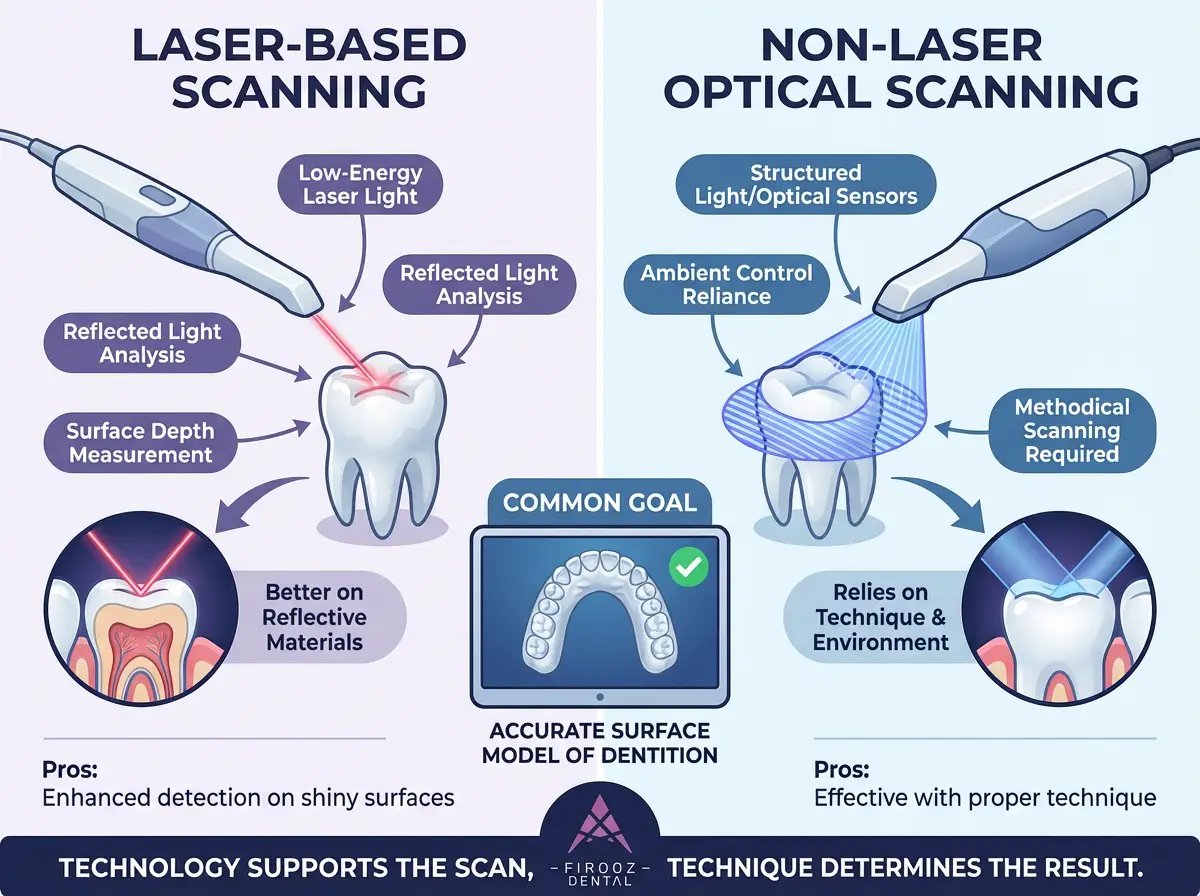
From a clinical standpoint, the distinction is less dramatic than marketing language often suggests. Both laser-based and non-laser optical scanners aim to achieve the same result: an accurate surface model of the dentition.
That said, there are practical considerations:
In real-world use, factors such as moisture control, operator training, and scanning strategy usually have a greater impact on scan quality than the light source itself.
No single optical method performs best in every clinical situation. Variations in arch length, restorative materials, soft tissue exposure, and patient movement all influence scan outcomes. Different technologies exist because they balance these variables in different ways.
For clinicians, the key takeaway is simple:
Understanding how these systems work helps set realistic expectations and leads to more consistent outcomes in daily practice.
In modern intraoral scanners, AI is used to support the clinician by improving how scan data is interpreted, not by making clinical decisions. During scanning, AI-based functions help recognize tooth surfaces, identify margins, and separate teeth from soft tissue by analyzing patterns in the captured surface data. For example, when minor gaps appear due to saliva or brief loss of tracking, the software can assist in smoothing transitions or flagging areas that need to be rescanned. In restorative cases, AI-assisted margin detection can help outline preparation edges more clearly, reducing manual adjustment time, but the final evaluation still depends on the clinician’s judgment. It is important to understand the limits of this approach: AI cannot correct poor scanning technique, compensate for inadequate isolation, or determine clinical suitability on its own. In daily practice, these tools are most effective when used as aids that reduce repetitive manual tasks while leaving control and responsibility firmly with the operator.
In restorative dentistry, intraoral scanners are most commonly used to record digital impressions for crowns, bridges, veneers, inlays, and onlays. The primary clinical goal in these cases is to capture accurate surface detail of prepared teeth, adjacent structures, and occlusion so that restorations can be designed and fabricated without distortion or remakes.
When compared to conventional impression materials, digital impressions remove several common sources of error. Traditional materials can distort due to tray movement, uneven pressure, setting time variation, or removal from undercut areas. In contrast, an intraoral scan records the tooth surface directly, eliminating material-related deformation and reducing the likelihood of retakes.
From a workflow perspective, intraoral scanning changes how restorative cases move through the clinic and laboratory:
Accuracy plays a central role in restorative outcomes. For single-unit restorations and short-span bridges, properly performed intraoral scans provide surface detail that supports precise marginal adaptation and occlusal fit. In daily clinical use, this often translates to fewer adjustments at delivery and improved predictability. However, the quality of the final restoration still depends on preparation design, moisture control, and scanning technique. Digital impressions do not compensate for unclear margins or inadequate reduction, but they do make such issues visible earlier in the process.
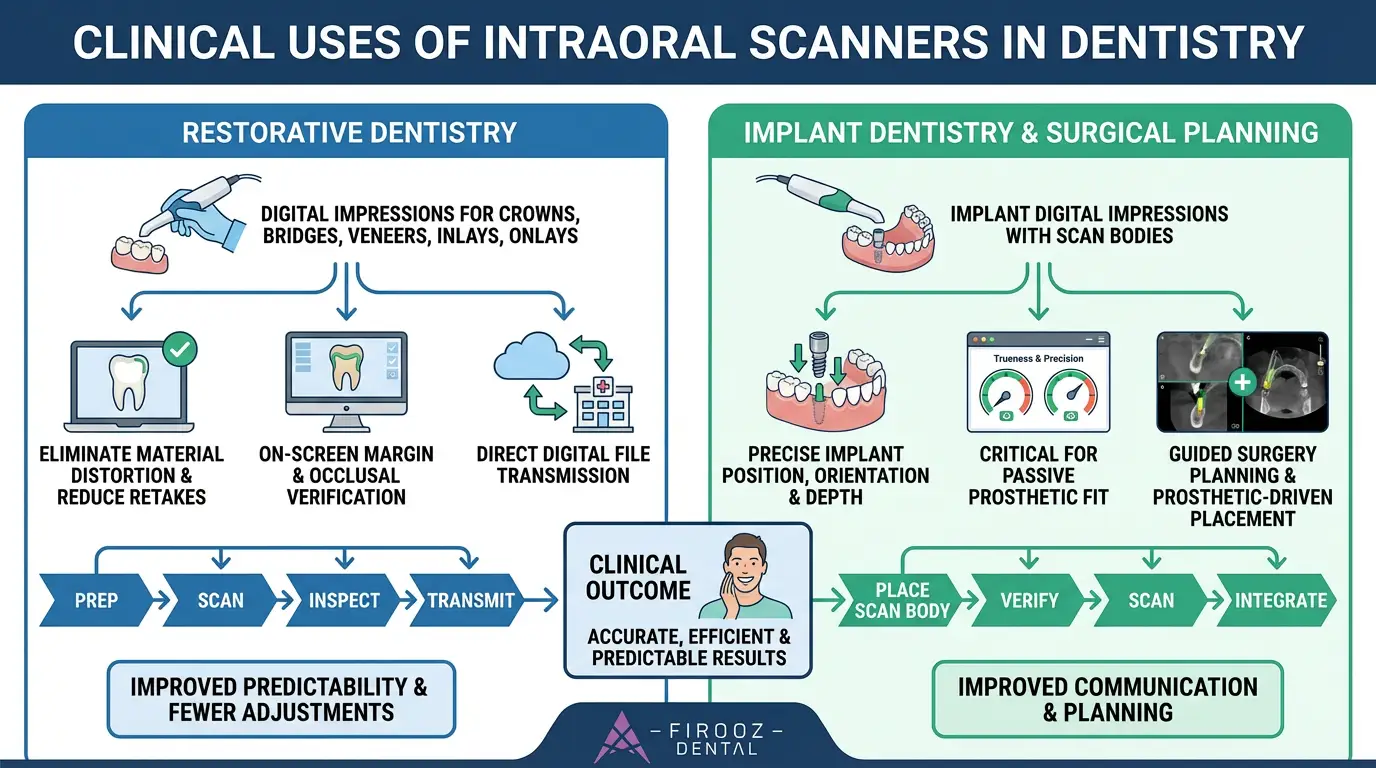
In implant dentistry, intraoral scanners are used to capture implant digital impressions through the use of scan bodies. A scan body is attached to the implant or abutment and serves as a reference marker that allows the software to identify implant position, orientation, and depth within the digital model. The accuracy of this step is critical, as even small positional errors can affect the fit of implant-supported restorations.
The implant scanning workflow typically includes:
In implant cases, trueness and precision are especially important. Trueness refers to how closely the scan represents the actual implant position, while precision refers to how consistently that position can be reproduced. Unlike tooth-supported restorations, implants lack periodontal mobility, which means inaccuracies are not compensated biologically. As a result, scanning protocol has a direct effect on prosthetic fit.
There are also practical limitations that must be considered. Full-arch implant scans are more sensitive to cumulative alignment errors than short-span cases. Factors such as scan length, scan path, and surface continuity all influence results. For this reason, many clinicians follow structured scanning sequences and verify data carefully before finalizing the scan.
In surgical planning, intraoral scans are often combined with cone beam imaging to create a comprehensive digital record. The scan provides detailed surface anatomy, while the radiographic data provides information about bone structure. Together, these datasets support guided surgery planning and prosthetic-driven implant placement. When used correctly, intraoral scanning improves communication between the clinician, laboratory, and surgical planning software, while keeping control of clinical decisions firmly in the hands of the practitioner.
In orthodontics, intraoral scanners serve a different purpose than in restorative or implant dentistry. The primary value is not limited to a single impression, but lies in the ability to create consistent digital records over time. These records allow clinicians to evaluate tooth movement, treatment response, and appliance fit without relying on physical models or repeated impression materials.
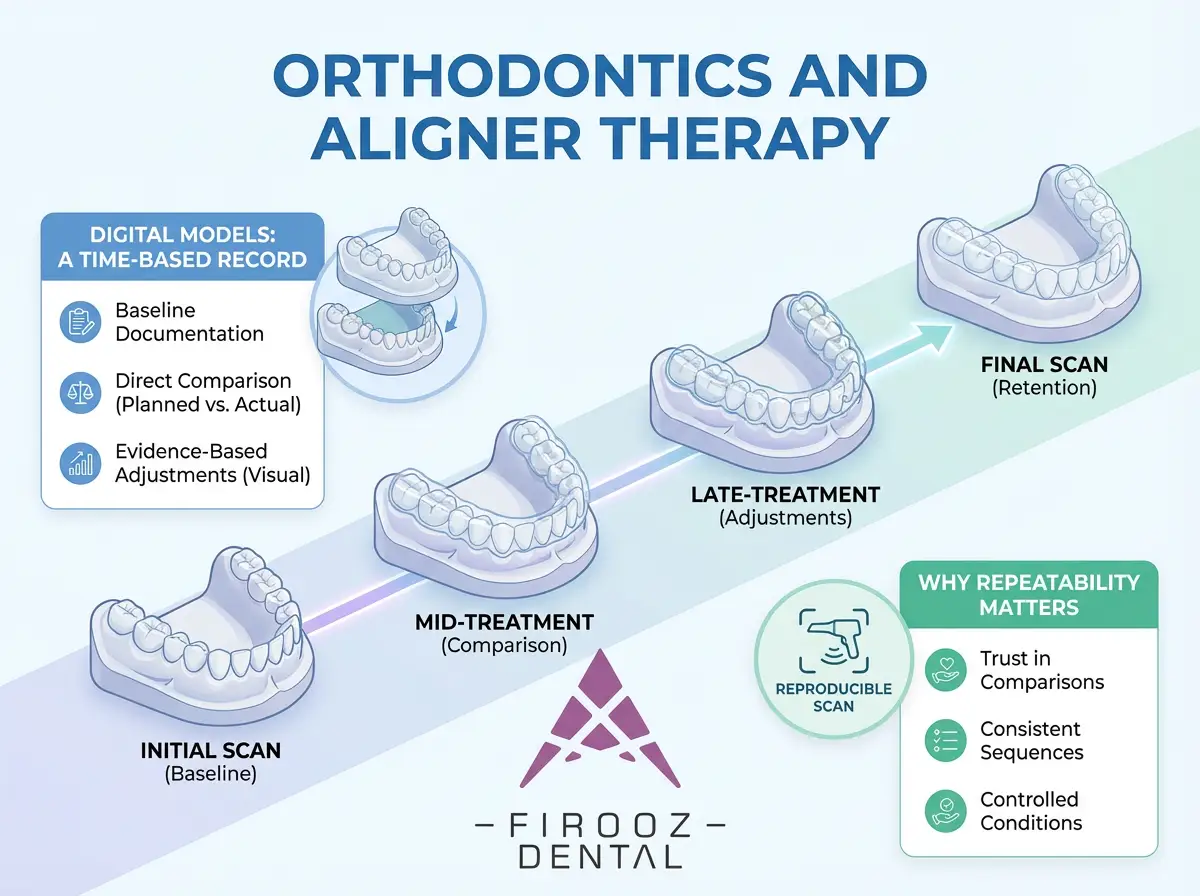
Each intraoral scan captures the dentition at a specific point in time. When scans are taken at regular intervals, they form a chronological sequence that reflects how teeth move throughout treatment. This approach supports orthodontic planning in several ways:
Because all models exist in the same digital reference space, small positional changes can be identified more clearly than with stone casts, which are difficult to compare accurately over time.
In orthodontic scanning, repeatability is often more important than how quickly a scan is completed. A scan that can be reproduced consistently under similar conditions allows clinicians to trust comparisons between visits. If scans vary due to inconsistent technique, differences in moisture control, or scanning path, it becomes difficult to determine whether observed changes reflect true tooth movement or scanning variation.
For this reason, orthodontic workflows tend to prioritize:
When these factors are maintained, intraoral scanning supports aligner therapy, fixed appliances, and retention monitoring with a level of clarity that traditional impressions cannot easily provide.
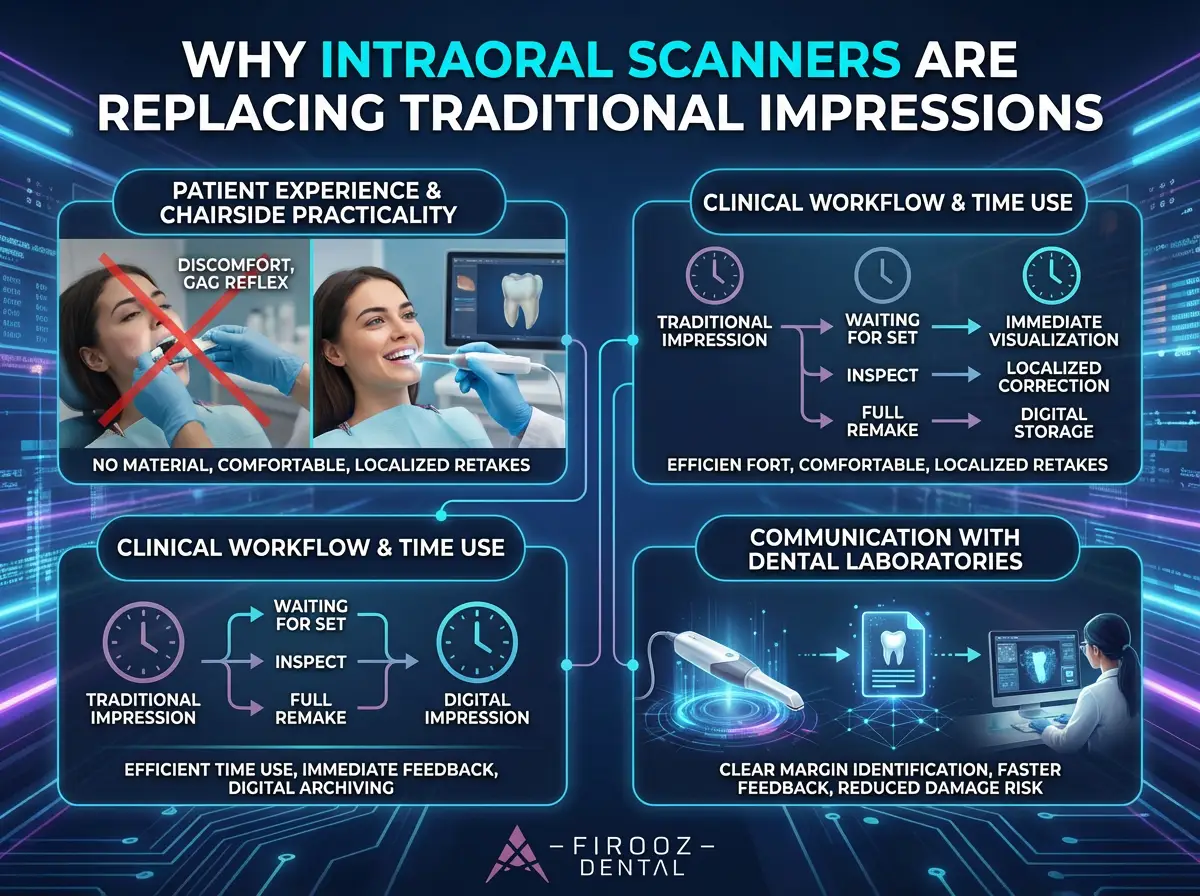
The shift from conventional impressions to digital scanning has not occurred because traditional methods failed, but because digital records address several long-standing clinical limitations. This transition affects patient experience, day-to-day clinical work, and communication with dental laboratories.
Don’t miss this video to compare traditional Impressions and intraoral scanning:
Patient Experience and Chairside Practicality
Conventional impressions often involve bulky trays, setting time, and discomfort, particularly for patients with strong gag reflexes or limited tolerance. Intraoral scanning replaces this process with a visual recording method that does not require impression material or tray placement.
From the patient’s perspective:
This change does not eliminate patient cooperation requirements, but it does reduce common sources of discomfort associated with traditional impressions.
Digital impressions alter how clinical time is spent rather than simply reducing it. Instead of waiting for materials to set and inspecting impressions after removal, clinicians can evaluate scan quality immediately.
Key workflow differences include:
However, scanning still requires training and attention. Poor scanning technique can result in incomplete data just as poor tray placement can lead to distorted impressions.
One of the most practical advantages of intraoral scanning is how information is shared with dental laboratories. Digital files provide a direct representation of the scanned surfaces and can be reviewed by both parties using the same visual reference.
This allows:
That said, digital files are only as useful as the data they contain. Clear preparation design and careful scanning remain essential.
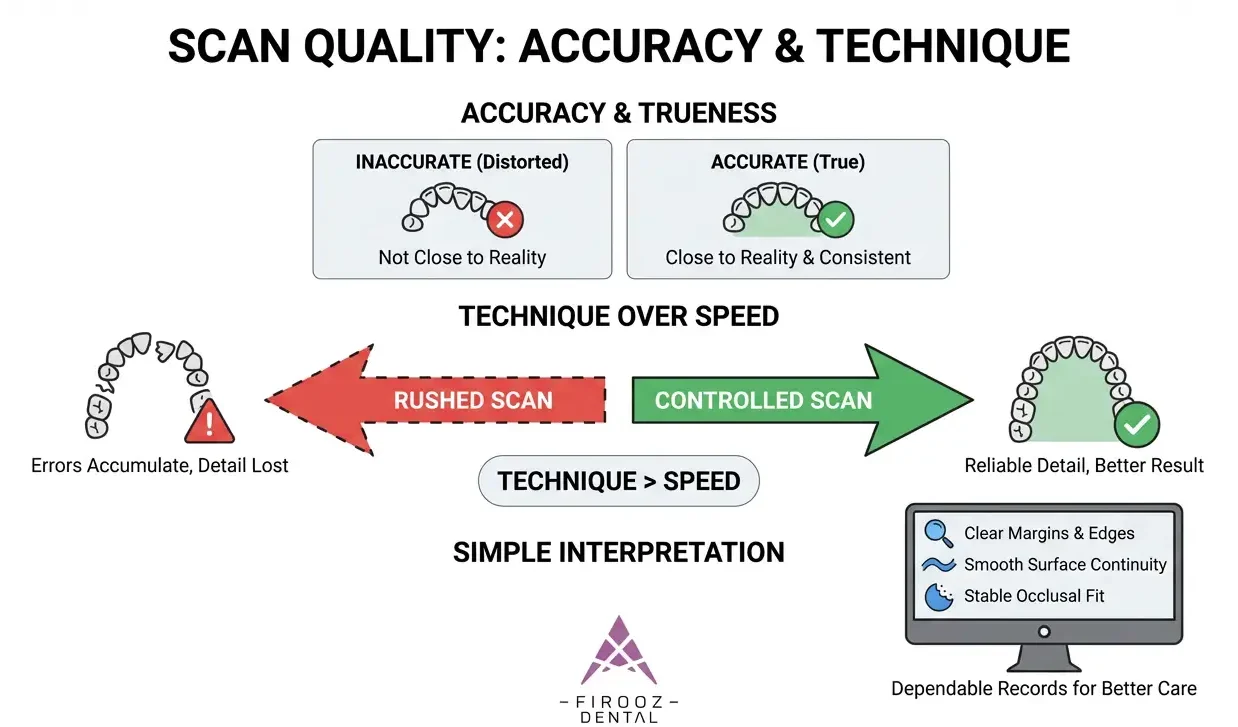
Terms like accuracy and precision are often used loosely in dentistry, but in digital scanning they have specific meanings that affect clinical outcomes. Understanding these concepts helps clinicians interpret scan quality more realistically.
In the context of intraoral scanning:
A scan can be precise without being true if it consistently reproduces the same error. Conversely, a scan can be close to reality but inconsistent if technique varies.
A fast scan is not necessarily a correct scan. When scanning is rushed, overlapping data may be insufficient, alignment errors may accumulate, and surface detail can be lost. In longer scans, especially full-arch cases, small misalignments can compound and affect the final model.
Clinical factors that influence scan reliability include:
Scientific literature consistently shows that scan quality depends more on controlled technique than on scan duration alone. For clinicians, this means that careful scanning habits matter more than completing the scan quickly.
In everyday practice, digital scans should be evaluated visually and contextually. Clear margins, smooth surface continuity, and stable occlusal relationships are more meaningful indicators than numerical values provided by software interfaces.
When used with proper technique and realistic expectations, intraoral scans provide dependable digital records that support diagnosis, planning, and communication across dental disciplines.
While intraoral scanners are widely used in daily practice, they are not without limitations. Understanding these challenges helps clinicians use digital impressions more effectively and avoid unrealistic expectations.
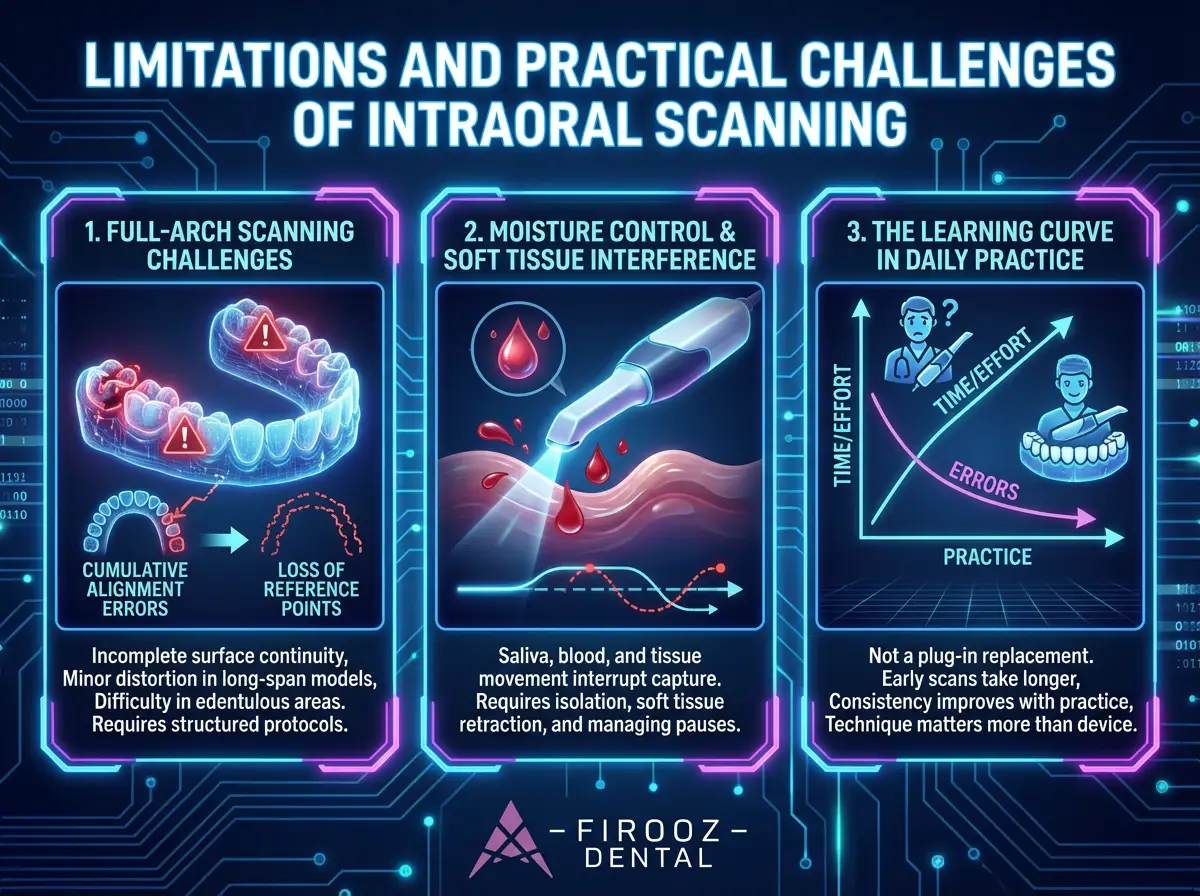
Full-arch scans are among the most demanding applications of intraoral scanning. Unlike short-span restorations, long scanning sequences increase the risk of cumulative alignment errors. Small inconsistencies in scanning path or surface overlap can add up, especially when reference points are lost across the arch.
Common issues in full-arch scans include:
These challenges do not make full-arch scanning unreliable, but they do require structured scanning protocols and careful review before finalizing the scan.
Moisture remains one of the most frequent sources of scanning difficulty. Saliva, blood, and soft tissue movement can interrupt surface capture and create gaps or irregular areas in the digital model.
From practical experience, scan quality improves significantly when:
Digital impressions reduce material-related distortion, but they do not remove the need for proper clinical control.
Intraoral scanning is not a plug-in replacement for conventional impressions. There is a learning curve, particularly in understanding scanning paths, overlap requirements, and software feedback.
Most clinicians report that:
With time and structured practice, scanning becomes predictable, but early training and realistic expectations are important for long-term success.
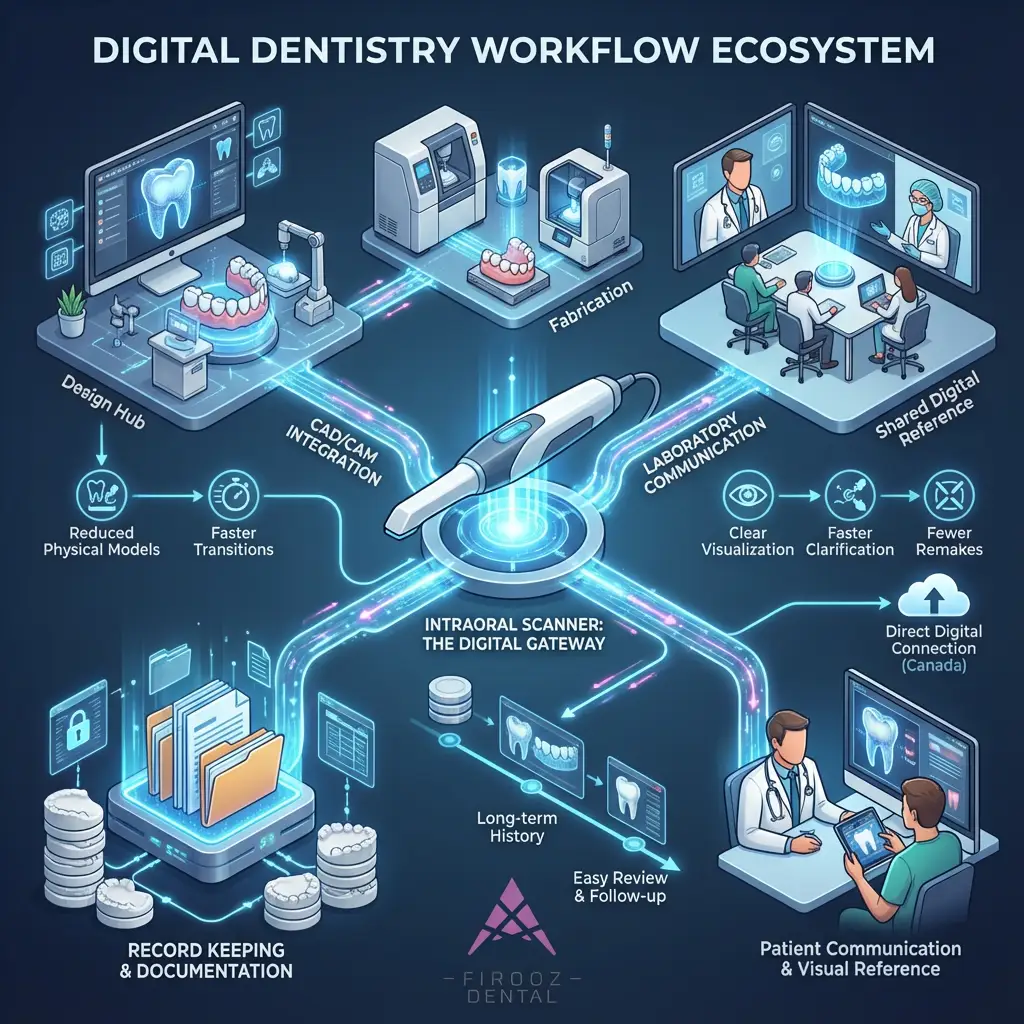
Intraoral scanners are not standalone devices. Their real value appears when they are integrated into broader digital dentistry workflows that connect clinical care, laboratory fabrication, and record management.
Digital impressions captured by intraoral scanners are commonly used as the starting point for CAD/CAM workflows. Once the scan is finalized, it can be imported directly into design software for restorative or orthodontic planning.
This integration allows:
For Canadian clinics that rely on external dental laboratories, this direct digital connection reduces delays related to shipping and remakes.
One of the most practical benefits of intraoral scanning is improved communication with laboratories. Both the clinic and the lab work from the same digital reference, which reduces interpretation errors.
In routine use, this supports:
Digital files also allow laboratories to review scans before fabrication begins, making it easier to identify issues early rather than after delivery.
Digital scans serve as long-term clinical records. Unlike physical models, they do not degrade, break, or require storage space. Over time, they provide a clear visual history of the patient’s dentition.
In modern Canadian practices, this supports:
As patient expectations continue to shift toward transparency and visual explanation, digital records play an increasingly practical role in daily care.
Intraoral scanners have changed how dental impressions are captured, reviewed, and shared, but their value lies in how they are used rather than in the technology itself. When applied with proper technique, realistic expectations, and good clinical control, digital impressions support accurate records, clearer communication, and more predictable workflows across restorative, implant, and orthodontic care.
At the same time, digital scanning does not remove the need for sound preparation design, moisture control, or operator skill. Full-arch cases, soft tissue management, and scanning consistency remain important considerations. For dental practices in Canada, intraoral scanners are best viewed as practical clinical tools that fit into a broader digital workflow tools that support decision-making, documentation, and collaboration when used thoughtfully and with attention to detail.
2 Responses
good article
thanks